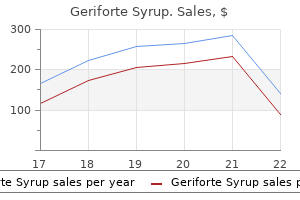
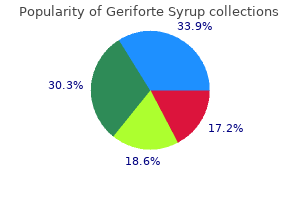
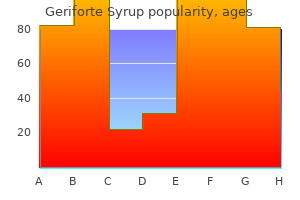
Geriforte Syrup
Geriforte Syrup
Geriforte Syrup dosages: 100 caps
Geriforte Syrup packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles

Ultrasonic estimation of fetal weight must herbals amla shikakai reetha shampoo buy discount geriforte syrup 100 caps on-line keep in mind whether or not or not the mom has diabetes herbs that lower blood sugar 100 caps geriforte syrup discount amex. However herbals a to z buy generic geriforte syrup 100 caps line, due to scant long-term follow-up, the prevalence of the permanency of the injury has not been properly established. Regression analysis demonstrated an affiliation between diabetes and cesarean supply that was not a results of toddler size alone. The strongest reported associations had been related to disproportion, earlier cesarean supply, failed induction, and malpresentation. These results and those from different studies suggest that the physician follow patterns and not macrosomia are the contributors to the excessive cesarean section rates. Most importantly, there have been no important variations between the two teams in the incidence of shoulder dystocia, preeclampsia, pelvic lacerations, or extended hospitalization, and the one two ruptured uteri occurred within the management group. In the earlier cesarean section group, the speed of repeat cesarean part doubled (56. Attempted supply at time period will lead to lower cesarean part rates than when being pregnant progresses and fetal weight estimation is >4000�4250 g. However, inadequate knowledge can be found to justify recommending either for or in opposition to induction of labor at term in pregnancies sophisticated by diabetes. Thus, the practitioner who elects to induce labor for his/her patient is properly advised to observe the identical old precautions taken by attendant on inductions for all pregnancies: taking special care to follow maternal glucose and Pitocin administration during labor; have the suitable personnel and equipment available for the administration of attainable shoulder dystocia. Confounding Factors There is paucity of data on the risks and advantages of induction of labor for pregnancies compromised by diabetes. Any plan of management for the induction of labor of a pregnant diabetic girl will want to resolve the confounding problems with cervical ripeness, labor management, epidural anesthesia, fetal body composition, and weight distribution and estimates of fetal weight. A giant matched cohort study79 compared the outcomes of labor between induced and spontaneous labor. Patients have been matched for nulliparity, cephalic presentation, time period gestation age, and precise delivery weight between 3800 g and 4000 g. In the induced group, there was a higher incidence of cesarean delivery (for dystocia and nonreassuring fetal heart price tracings) and increased instrumental deliveries. In our examine,80 evaluating induction of labor with spontaneous labor, the affect of cervical status at the onset of induction was addressed. Women with a Bishop score81 7 acquired vaginal prostaglandin as a cervical ripening agent. Regardless of the initial Bishop score, girls present process labor induction and ripening of the cervix had the next cesarean part price than those with spontaneous supply. There had been no statistically significant variations between the misoprostol or placebo groups with regard to the Bishop rating. A risk-scoring system was used to information the frequent use of preventive labor induction in one hundred nulliparous women. The start outcomes of this group have been compared with these of 352 nulliparous girls who received traditional care. The Adverse Outcome Index and the rate of uncomplicated vaginal delivery were used to measure overall birth health. They concluded that publicity of nulliparous girls to a excessive preventive induction price was significantly related to improvement in delivery well being. Although several research have examined induction of labor for the indication of estimated macrosomia in nondiabetic women,84�87 there have been few studies carried out solely on pregnancy sophisticated by diabetes. Patients had been assigned both to elective supply at 38 weeks or to expectant administration, which included twice weekly cardiotocography and amniotic fluid quantity analysis. Because of the paucity of studies, they determined that both elective supply at 38 weeks or expectant management is comparable. In one other research,90 insulin-requiring well-controlled type 2 and gestational diabetic women had been randomized to both induction of labor or expectant administration at 38 weeks. The imply gestational age difference between groups at delivery was 1 week and the imply difference in delivery weight was 226 g. With the belief that diabetic infants acquire 40�60 g every day (50 g � 7 days = 350 g), no difference was discovered between the 2 groups. In the trial of labor instances that resulted in vaginal deliveries, the rate of recurrence of shoulder dystocia was high-approximately 10 occasions greater than the speed for the final population. There is scant data reporting the association between labor abnormalities, induction of labor, and shoulder dystocia. The low forceps group had two- to threefold higher rates of shoulder dystocia in normal and irregular labor together with prolonged latent section, protraction disorder and arrest dysfunction. The price of shoulder dystocia was roughly twofold greater within the price class >4500 g in comparability to infants weighing 4000�4499 g. However, even in the decrease weight category, the rate of shoulder dystocia was 15%�38% relying on the labor abnormality. In another examine, a significant association was discovered between active-phase abnormalities and shoulder dystocia however it included only 36 sufferers. The research found considerably greater rates of shoulder dystocia in induction of labor. This may partly be as a outcome of fetal size that itself is associated with shoulder dystocia. Therefore, labor augmentation with cautious monitoring the Pitocin administration should be the strategy of choice in the presence of fetal macrosomia rather than routine cesarean supply. However, several conditions, corresponding to maternal obesity, previous and present macrosomia, earlier shoulder dystocia, labor abnormality, induction of labor, and instrumental supply are probably suspects for an impending shoulder dystocia that should set off "anticipatory alarms" for the obstetrician. In our study68 when practitioners have been "asleep on the watch," in circumstances not identified as macrosomic by ultrasound exam, the rate of shoulder dystocia was 19%. Several authors43�45,91�93 sought to consider supply mode administration choices and the rate of shoulder dystocia recurrence for ladies with a prior supply difficult by shoulder dystocia. One study91 included all vaginal deliveries sophisticated by shoulder dystocia from 1996 to 2001. The obstetrician must master the commonest maneuvers in order that beneath duress, the maneuver turns into computerized, efficient, and hopefully efficient. In our study, we found that 45% of the shoulder instances can be launched with one maneuver, 39% with two, and 11% with three. Finally, when the conventional maneuvers fail to release the shoulder, the Zavanelli maneuver (cephalic replacement) is a possible option. If corkscrewing nonetheless leaves you colder, Then gently ship the posterior shoulder. Unless obstetric complications dictate otherwise, the uncomplicated (normal estimated delivery weight, amniotic fluid quantity, and metabolic control) diabetic pregnancy, each pregestational and gestational, can be allowed to go into spontaneous supply at full term. This will result with a comparatively giant number of patients who can endure spontaneous vaginal delivery somewhat than being electively induced with the accompanying threat for this process. The affiliation between stillbirth in the first pregnancy and subsequent adverse perinatal outcomes. Identifying the causes of stillbirth: a comparison of four classification techniques. Cause of dying in infants of women with pregestational diabetes mellitus and the connection with glycemic management. Diabetic embryopathy: studies utilizing a rat embryo culture system and an animal model. Elevated ranges of endothelin-1 and prostaglandin E2 and their impact on nitric oxide generation in placental tissue from neonatal streptozotocin-induced diabetic rats. Gestational diabetes mellitus diagnoses with a 2-h 75-g oral glucose tolerance check and antagonistic pregnancy outcomes. The management of being pregnant complicated by diabetes and of children of diabetic moms. The risk of stillbirth and infant death stratified by gestational age in girls with gestational diabetes. Neonatal outcomes after demonstrated fetal lung maturity earlier than 39 weeks of gestation. Categorization of terminal fetal heart-rate patterns in antepartum cardiotocography. The growth restriction intervention trial: long-term outcomes in a randomized trial of timing of supply in fetal progress restriction. The association between birthweight 4000 g or larger and perinatal outcomes in sufferers with and with out gestational diabetes mellitus. Shoulder dystocia: ought to the fetus weighing 4,000g be delivered by cesarean section
Note that herbals for hair growth discount geriforte syrup 100 caps without a prescription, according to delicate cirrhosis earthworm herbals generic geriforte syrup 100 caps without a prescription, there are fibrotic reticulations throughout the liver; these are most pronounced within the left lateral segment wicked herbals amped geriforte syrup 100 caps buy with amex. Patients with hereditary hemochromatosis could develop iron overload in the pancreas and myocardium. Gradient echoes are extra delicate to susceptibility effects than spin echoes, and the signal loss is more pronounced on gradient echo pictures. If iron overload is severe, the degree of signal loss could additionally be marked on each kinds of pictures. Although iron primarily shortens the T2 and T2* of the liver, it also shortens the T1, and the liver could have elevated sign depth on T1-weighted sequences acquired with very brief echo instances. Concomitant liver steatosis could confound the interpretation, nevertheless, as a result of fat-water part interference will alter the relative signal intensities of the in-phase and out-of-phase pictures. Alternatively, multiple gradient echoes could be obtained and the consequences of fat-water section interference and T2* relaxation modeled concurrently. Of the sequence of 12 photographs, 5 are presented for illustrative purposes with echo instances as proven. The T2* worth was calculated assuming monoexponential signal decay from the 12 echoes. The estimated T2 value, 45 ms, is simply barely lower than the conventional 50- to 60-ms T2 measured on this scanner. As shown on this instance, a given quantity of iron deposition causes larger T2* shortening than T2 shortening. T2-weighted and T2*-weighted pictures may show hypointensity in the pancreas and, if acquired with cardiac gating, the myocardium. Axial spoiled gradient recalled echo magnetic resonance photographs by way of the liver at echo times of 2. The hepatic findings are in keeping with hemochromatosis or secondary hemosiderosis. However, marked signal loss between echoes in the renal cortex (arrows) signifies renal parenchymal iron deposition. Co-localized spoiled gradient recalled echo magnetic resonance photographs acquired at echo instances of two. The liver parenchyma progressively loses sign as echo time increases, consistent with short T2* rest. These siderotic nodules have greater concentrations of iron than the rest of the liver. If gradient echoes are used for T2* measurements, it is necessary to cut back possible phase-interference effects from concomitant fat accumulation by acquiring echoes only at in-phase echo times or acquiring pictures with frequencyselective fat saturation (or water excitation). A decreased signal intensity ratio of liver to paraspinal muscle has been shown to have excessive sensitivity and specificity for Document t�l�charg� de ClinicalKey. The exact ratio used for diagnostic classification depends on the imaging parameters of the sequence. Uptake of sulfur colloid by the siderotic liver could also be reduced secondary to Kupffer cell damage incurred from iron overload. The colloid scan may be abnormal, however the alteration tends to be gentle and may be tough to appreciate. If relaxometry is unavailable, liver-to-muscle signal intensity ratio measurements may suffice. T2*-weighted imaging and in-phase and out-of-phase imaging are helpful for detecting the presence of iron. Multiple echo T2 and T2* relaxometry and liver-to-muscle signal intensity ratios additionally can be utilized to grade the degree of iron overload. T2 and T2* values obtained using one protocol may not be reproducible utilizing different protocols. Differential Diagnosis the clinical differential prognosis of hereditary hemochromatosis makes an attempt to distinguish between primary (genetic) and secondary (acquired) causes of iron overload. Secondary causes of hepatic iron overload are dominated out if genetic testing suggests a major trigger. History and evaluation of laboratory exams establish these with transfusional iron overload and iron-loading anemias. In addition, most secondary causes of hepatic iron overload are characterized histologically by iron deposition within Kupffer cells rather than hepatocytes. Histologic examination also might provide proof for a selected underlying disease. In hereditary hemochromatosis, iron overload is restricted to the liver early in the course of illness, with subsequent involvement of the pancreas and myocardium. The reticuloendothelial organs (spleen, marrow, and lymph nodes) are relatively spared. By comparison, secondary hemosiderosis leads to uniform iron deposition in the reticuloendothelial system and in addition might involve the renal cortex. Patients with hepatic hyperattenuation as a outcome of glycogen storage illness could present with large hepatomegaly as properly as a number of hepatic adenomas. Iron chelation agents, corresponding to deferoxamine, are used with modest success in patients with secondary hemosiderosis. If profitable, discount in hepatic iron concentrations with chelation therapy considerably reduces the danger for clinical disease attributable to iron overload in these patients. Asberg A, Hveem K, Thorstensen K, et al: Screening for hemochromatosis: high prevalence and low morbidity in an unselected population of 65,238 individuals. Guyader D, Jacquelinet C, Moirand R, et al: Noninvasive prediction of fibrosis in C282Y homozygous hemochromatosis. Beaton M, Guyader D, Deugnier Y, et al: Noninvasive prediction of cirrhosis in C282Y-linked hemochromatosis. As genetic situations, their manifestations are wideranging and systemic, with hepatic involvement just one component of the bigger illness. The commonest of these problems, hereditary hemochromatosis, is discussed in detail in its personal chapter on hepatic iron overload. Hepatocytes then excrete the copper into bile, leading to biliary copper excretion, which finally results in fecal copper loss. Unincorporated copper accumulates inside hepatocytes, the place it causes secondary oxidative tissue harm. Some of the excess copper enters the systemic circulation and is deposited in extrahepatic sites such as the mind (especially the basal ganglia and limbic system), cornea, and kidneys. Ceruloplasmin not integrated with copper is released into the bloodstream and rapidly degraded. Its most important physiologic position is to inactivate proteolytic enzymes in the lung (especially neutrophil elastase), which degrade lung matrix tissue after being launched as a by-product of cellular immune responses to airborne pathogens. It is characterized by progressive neurologic deterioration and persistent liver disease leading to cirrhosis. Highly expressed within the liver, kidney, and placenta, it encodes a metal-transporting, copperdependent P-type adenosine triphosphatase that capabilities within the incorporation of copper into ceruloplasmin (plasma protein that binds copper) and excretion of excess copper into bile. The continual kind develops over a period of many years, ultimately leading to the everyday findings of cirrhosis and complications of portal hypertension. Neuropsychiatric symptoms are the initial manifestation in 40% to 50% of patients. Serum aminotransferase levels are sometimes mildly elevated (<200 international units/L), with a proportional increase in whole bilirubin (<4. In some cases, liver biopsy is indicated with consideration positioned on the hepatic copper content material. Pulmonary illness is accelerated by noxious stimuli, similar to tobacco and air pollutants. Cirrhosis develops slowly, usually requiring 20 to 30 years for portal hypertension to happen, and is the most common stage of presentation. Patients might exhibit complications of portal hypertension, together with variceal bleeding, hypersplenism, ascites, and hepatic encephalopathy. The mean life span is sixty five years in nonsmokers and is reduced to 50 years in smokers. Seventy % of sufferers are identified earlier than the age of two years, with the event of hepatic adenomas within the second decade of life. The presentation may be either acute or chronic; acute disease sometimes manifests as fulminant hepatic failure, whereas continual disease consists of continual hepatitis, cirrhosis, and neuropsychiatric illness. Those presenting with hepatic disease usually will develop neuropsychiatric signs within 2 to 5 years.
The major advantages of radionuclide cystography include its higher sensitivity herbals shoppes geriforte syrup 100 caps buy discount online, because of steady imaging throughout bladder filling and voiding with much less reflux required for visualization herbals during pregnancy geriforte syrup 100 caps buy generic on line, and significantly lower radiation dose herbals benefits purchase geriforte syrup 100 caps otc, significantly gonadal dose. B, the voiding urethrocystogram in the identical affected person demonstrates high-grade vesicoureteral reflux. Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Jakobsson B, Nolstedt L, Svensson L, et al: 99mTechnetium-dimercaptosuccinic acid scan within the analysis of acute pyelonephritis in youngsters: relation to scientific and radiological findings. A smaller percentage of approximately 20% are related to tuberous sclerosis complicated, and it might possibly occur in as many as 55% 75% of patients with it. In a minority of cases, signs such as flank pain, nausea, vomiting, and fever are produced by mass effect and intratumoral or perirenal hemorrhage. Pathophysiology Isolated angiomyolipomas are often solitary, whereas angiomyolipomas associated with tuberous sclerosis are sometimes multiple, larger, and bilateral. On gross examination, angiomyolipomas are composed predominantly of fats and have a homogeneous yellow look. Tumors with more various proportions of fats, smooth muscle, and blood vessels have a heterogeneous gross pathologic appearance. However, when a big fats part is current, the imaging characteristics are normally pathognomonic and vice versa. Intravenous urography and plain radiography are typically not delicate methods for figuring out these tumors. The sonographic criteria for a simple cyst are well established and embrace (1) anechoic contents, (2) sharp clean partitions, (3) posterior acoustic enhancement, and (4) lack of inner blood move. The majority of angiomyolipomas are sporadic (80%) and are sometimes identified in adults, with a robust female predilection as compared 750 Document t�l�charg� de ClinicalKey. Typically, the lesion is a well-defined, cortical, heterogeneous mass with a fats part. Soft tissue attenuation of the lesion could additionally be because of hemorrhage, easy muscle, or fibrosis. These lesions can also show distinction enhancement because of the relatively bigger smooth muscle and vascular components. In the presence of serious calcification, the prognosis of angiomyolipoma should be reconsidered. Variable areas of excessive signal are seen on T1and T2-weighted images owing to the fat content. However, high signal intensity on T1-weighted photographs also may be seen with high protein content material or hemorrhage. When surgical administration is indicated, it can be used to assess differential renal perform. Angiography characteristically demonstrates clusters of saccular microaneurysms or macroaneurysms. A, T1-weighted magnetic resonance image exhibits a hyperintense lesion arising from the posterior left kidney. Treatment When lesions are small, asymptomatic, and found by the way, no remedy is important. Larger lesions if thought-about at risk for hemorrhage may be prophylactically embolized. In severe acute presentation, complete nephrectomy could additionally be required if conservative measures fail. Ultrasound picture exhibits a spherical echogenic construction within the upper pole of the kidney. An oncocyte is a big remodeled epithelial cell with a finely granular eosinophilic cytoplasm. They average 7 cm in diameter and are most often symptomatic when bigger than 5 cm. Plain radiographic findings are nonspecific and embrace a gentle tissue mass distorting the renal silhouette with displacement of the fats planes. The basic findings are a spokewheel association of vessels, homogeneous dense tumor blush in the course of the capillary section, and sharp demarcation from the kidney. An oncocytoma sometimes seems as a well-defined solid renal mass with smooth margins. Typically, oncocytoma demonstrates low sign on T1-weighted pictures and high signal on T2-weighted photographs. After administration of a contrast agent, oncocytoma typically demonstrates homogeneous enhancement. Evaluation for vascular involvement, lymphadenopathy, and extent of the lesion is feasible Table 63-2). Consequently, many clinicians select pathologic sampling with partial or whole nephrectomy. Less widespread signs and symptoms embrace hematuria, hypertension, vomiting, and hypercalcemia. This variant has a poorer prognosis and is often seen in infants and youngsters older than 3 months of age. A strong, homogeneous mass arising from the kidney which will exchange all or a half of the involved kidney. However, entrapment of nephrons inside the mass might trigger excretion of contrast agent inside the mass. There is low sign intensity on T1-weighted imaging, and the tumor is typically nonenhancing. Prenatal or pediatric ultrasonography is often the first imaging examine performed when the stomach mass is palpated. There is a female predominance, and sufferers are younger than those with essential hypertension. Occasionally, acute flank pain, hypotension, and anemia secondary to tumor hemorrhage are famous. Most are situated beneath the renal capsule, though they could arise close to the renal pelvis. They are sharply defined with a pseudocapsule and commonly comprise foci of hemorrhage inside them. Lack of calcification makes these tumors tough to establish on plain radiographs. Treatment Patients with the aggressive variant could profit from adjunctive chemotherapy or irradiation. Pathophysiology Adenomas are small, well-differentiated tumors of the renal cortex. Most of those lesions are identified at post-mortem and are subsequently of little scientific significance. Less commonly, patients present with symptoms of metastatic illness, corresponding to bone ache. Patients also might present with systemic symptoms of malignancy such as fatigue, weight loss, and fever. A well-described presentation in men is new unilateral (usually left) varicocele secondary to compression or obstruction of the ipsilateral renal vein by tumor or thrombus. The 5-year survival of papillary and chromophobe subtypes (80% to 90%) is significantly greater than for clear cell subtype (50% to 60%). Renal medullary carcinoma is extraordinarily aggressive, and metastases, particularly to regional lymph nodes, are generally current at prognosis. Environmental threat elements embrace smoking; unopposed estrogen publicity; obesity (particularly in women); occupational publicity to petroleum merchandise, heavy metals, and asbestos; and hypertension and its treatment. Bilateral or multifocal tumors are seen in approximately 5% of sporadic circumstances, typically with equivalent histologic subtype within the multiple tumors. A, Scout tomogram from a computed tomography scan exhibits calcification in the left higher quadrant (arrow). Axial contrast-enhanced (B) and coronal unenhanced (C) pictures present the irregular pattern of calcification associated with this tumor arising from the anterior side of the decrease pole of the left kidney.
In cardiac arrest herbals on demand reviews 100 caps geriforte syrup purchase with amex, restoration of output is often followed by adrenaline-induced hypertension bajaj herbals geriforte syrup 100 caps order on line. When given to conscious sufferers in anaphylaxis or in an try to banjara herbals geriforte syrup 100 caps cheap produce native vasoconstriction, it usually causes anxiousness, tremor, headache and palpitations. It may trigger angina, myocardial infarction and arrhythmias, particularly in patients with current heart illness. When given to induce native vasoconstriction, it ought to be used with caution in patients with heart disease. When administered with an area anaesthetic to induce native vasoconstriction, a readymixed adrenaline�anaesthetic preparation should be used; normally this incorporates adrenaline at a concentration of 1: 200,000 (5 micrograms/mL) together with the anaesthetic. In cardiac arrest, adrenaline is run from a pre-filled syringe containing a 1: 10,000 (1 mg in 10 mL) answer. Inject this into the anterolateral facet of the thigh midway between the knee and the hip, from the place it ought to be rapidly absorbed. In the context of cardiac arrest and anaphylaxis, intensive scientific and haemodynamic monitoring is important. Administration Communication Monitoring Cost Clinical tip-The use of a local anaesthetic blended with adrenaline often induces a gentle however fairly unpleasant sensation of tension for the patient. The use of adrenaline in this context is probably most acceptable in the operating theatre, the place it can be injected while the affected person is beneath common anaesthesia as a way of prolonging post-operative analgesia. This increases the reabsorption of sodium and water (which elevates blood pressure) with the by-product of elevated potassium excretion. Aldosterone antagonists inhibit the effect of aldosterone by competitively binding to the aldosterone receptor. Their effect is greatest in major hyperaldosteronism or when circulating aldosterone is increased. An essential opposed impact of aldosterone antagonists is hyperkalaemia, which can lead to muscle weak point, arrhythmias and even cardiac arrest. Spironolactone causes gynaecomastia, which can have a significant influence on affected person adherence (see Communication). Aldosterone antagonists could cause liver impairment and jaundice and are a explanation for Stevens�Johnson syndrome (a T cell-mediated hypersensitivity reaction) that causes a bullous skin eruption. Aldosterone antagonists can cross the placenta throughout being pregnant and appear in breast milk so ought to be avoided the place potential in pregnant or lactating girls. Nevertheless, when supported by acceptable monitoring, this can be a useful combination in the context of coronary heart failure. Spironolactone is used for all indications, whereas epleronone is just licensed for the treatment of heart failure. Aldosterone antagonists ought to be prescribed for normal administration, usually as a single daily dose. You ought to tailor the dose to the particular indication as, for instance, much larger doses are used to treat ascites secondary to cirrhosis than are used in heart failure. A typical starting dose of spironolactone is one hundred mg day by day for ascites in comparability with 25 mg daily for heart failure. Spironolactone can be out there as a combined preparation with a thiazide or loop diuretic. Reassure them that such effects are benign and reversible, however acknowledge that they could be uncomfortable and embarrassing. Advise all sufferers that aldosterone antagonists could cause their potassium degree to rise and reinforce the importance of attending for blood checks. Efficacy must be monitored by affected person report of signs and scientific findings. Safety ought to be monitored by checking renal perform and serum potassium concentration as a result of threat of renal impairment and hyperkalaemia. Administration Communication Monitoring Cost Clinical tip-Spironolactone is a comparatively weak diuretic that takes several days to begin having an impact. It is due to this fact often prescribed together with a loop or thiazide diuretic, where it both counteracts potassium losing and potentiates the diuretic impact. For example, in the therapy of ascites because of continual liver failure, spironolactone and furosemide are typically used collectively in a ratio of about 5: 1. These medicine are most often taken as compound preparations containing an alginate with a number of antacids, such as sodium bicarbonate, calcium carbonate, magnesium or aluminium salts. Alginates act to increase the viscosity of the stomach contents, which reduces the reflux of stomach acid into the oesophagus. Antacids alone (usually aluminium or magnesium compounds) can be used for the short-term relief of dyspepsia. Compound alginates cause few side effects, which vary relying on their constituents and the dose taken. Magnesium salts can cause diarrhoea, whereas aluminium salts can cause constipation. Sodium- and potassiumcontaining preparations ought to be used with caution in sufferers with fluid overload or hyperkalaemia. Some preparations include sucrose, which might worsen hyperglycaemia in people with diabetes mellitus. The divalent cations in compound alginates can bind to different medicine, decreasing their absorption. Antacids can scale back serum concentrations of many medication, so the doses ought to be taken at completely different occasions. By growing the alkalinity of urine, antacids can enhance the excretion of aspirin and lithium. Check the constituents of the model chosen, notably if prescribing for patients with renal impairment or diabetes mellitus. Explain that the medication should relieve the symptoms of heartburn and acid indigestion inside about 20 minutes and for several hours afterwards. Discuss lifestyle measures that can be taken to scale back reflux, such as eating smaller meals more typically, figuring out and avoiding foods and drinks triggers, stopping smoking and raising the pinnacle of the bed. Advise them to depart a gap of no less than 2 hours between these medicines and other medicine that they could intact with (see Interactions). Symptomatic response should be monitored by the patient and their healthcare practitioner. Administration Communication Monitoring Cost Clinical tip-Compound alginates are a useful therapy in the armamentarium of the paediatrician. Around 10�20% of kids endure from gastro-oesophageal reflux illness, and compound alginates have been shown to reduce frequency of signs. Inhibition of xanthine oxidase lowers plasma uric acid concentrations and reduces precipitation of uric acid in the joints or kidneys. The most common side effect is a pores and skin rash, which may be delicate or could indicate a more severe hypersensitivity response corresponding to Stevens�Johnson syndrome or poisonous epidermal necrolysis. Drug hypersensitivity syndrome is a uncommon, life-threatening reaction to allopurinol that can embody fever, eosinophilia, lymphadenopathy and involvement of different organs, such as the liver and pores and skin. Recurrent skin rash or signs of more extreme hypersensitivity to allopurinol are contraindications to remedy. The dose ought to therefore be reduced in sufferers with extreme renal impairment or hepatic impairment. The cytotoxic drug mercaptopurine and its pro-drug azathioprine require xanthine oxidase for metabolism. When allopurinol is prescribed with these drugs, it inhibits their metabolism and will increase the risk of toxicity. Where allopurinol is used as a part of cancer treatment, it must be commenced before chemotherapy. Allopurinol ought to be taken after meals and sufferers must be inspired to keep good hydration with fluid consumption of 2�3 litres every day. Advise patients that the aim of remedy is to reduce assaults of gout (or formation of kidney stones). Explain that that is often delicate and goes away on stopping the drug, however it could be an indication of a extra critical allergy. Advise sufferers to not cease allopurinol if they get an acute attack of gout, as this might make the attack worse.
Acute gastrointestinal bleeding is less common than in small bowel adenocarcinoma bajaj herbals pvt ltd ahmedabad geriforte syrup 100 caps buy overnight delivery, however the danger for perforation is higher herbalsolutionscacom discount geriforte syrup 100 caps visa. As they improve in dimension herbs parts proven 100 caps geriforte syrup, the most typical manifesting symptom is gastrointestinal bleeding and belly pain. Carcinoid tumors are submucosal, are more frequent within the ileum, and produce a attribute mesenteric mass through lymphatic spread. Lymphoma of the small bowel might be either a major small bowel tumor or a manifestation of lymphomatous disease. Lymphoma can occur anywhere within the gastrointestinal tract however is extra frequent within the distal small bowel. On gross pathologic study, carcinoids are white, yellow, or grey firm nodules that hardly ever exceed 3. They can typically manifest as multiple nodules (30% of cases), exophytic masses, or intramural plenty. They may protrude into the lumen as polypoid nodules or classically manifest as infiltrative fibrous lesions. These are usually slow-growing tumors which will cause superficial ulcerations and hemorrhage. The metastatic deposits of carcinoid within the lymph nodes, mesentery, and liver range in measurement and gross morphology. Extensive involvement of the subserosa and adjoining mesentery stimulates local launch of serotonin, which is answerable for the event of desmoplastic response. Mesenteric arteries and veins positioned both close to and much from the tumor may be thickened and will end in intestinal ischemia. They can be characterized as benign, borderline, of low malignant potential, or malignant based mostly on the pathologic appearance. Currently, small bowel collection and enteroclysis are used for evaluation of small bowel tumors in detecting small lesions. Arrowheads point out the overhanging edges (shouldering) at both ends of the lesion. Contrast radiographic studies are important within the preliminary evaluation of small bowel diseases. Ulcerations may be well appreciated on small bowel collection as barium-filled craters on the floor of the lesion. The exophytic lesions can cause important mass impact on the adjoining bowel loops that can be evident on the plain movie. The tumor can immediately invade adjacent structures in the stomach and, if metastatic, can unfold to the liver and peritoneum. A, Spot film from enteroclysis reveals irregular narrowing of an ileal section (arrow) with kinking of the lumen and fixation of the loops. B, Mesenteric spiculated mass (arrow) and desmoplastic reaction in the small bowel mesentery (arrowheads) tethering adjacent small bowel loops are higher demonstrated on the axial computed tomography image. Well-defined polypoid lesion in the terminal ileum (arrow) is by the way noted on the peroral pneumocolon research. Circumferentially infiltrated lymphoma causing irregular narrowing of a jejunum segment (arrows). The highdensity oral contrast brokers can mix inconsistently with gastric and intestinal fluid, resulting in pseudotumors, and in addition obscure the enhancing bowel wall or enhancing tumors corresponding to carcinoid when the intravenous distinction agent is administered rapidly. Also, if 3D imaging of the small bowel or mesenteric vessels is deliberate, the utilization of high-density oral brokers will hinder the postprocessing protocol. These tumors can show indicators of necrosis, hemorrhage, and, occasionally, ulceration, as seen in 40% of instances. Dilated ileum phase with irregular contours (arrow), typical for lymphoma involvement. Thirty percent of carcinoid tumors are multicentric and might manifest as a quantity of nodules and ultimately extend into the adjacent mesentery. The mass has spiculated margins, low attenuation, and adjacent fats stranding and infrequently causes encasement of mesenteric vessels, leading to ischemia of the affected bowel loops. Fibrosis within the mesentery may create a "spokewheel" or "sunburst" appearance of mesenteric vessels. Infiltrative tumors can manifest as uneven mural thickening, producing fibrosis and subsequent malignant stricture. At the time of prognosis, 58% to 64% of sufferers with small intestinal carcinoids have illness that has spread past the gut to regional lymph nodes or the liver. A, Spot movie from small bowel follow-through reveals large excavated mass (arrows) displacing the adjoining small bowel loops. B, Axial computed tomography picture demonstrates the big mass (arrow) with homogeneously hypodense heart. Coronal (A) and axial (B) computed tomography images reveal focal irregular narrowing and concentric wall thickening in an ileum segment (arrows) representing adenocarcinoma, which was later confirmed by surgery. The tumor infiltrates the muscular layer of the wall and may develop aneurysmal dilatation of bowel loops. Small bowel lymphoma spreads via direct extension into adjoining organs or hematoge- nously to the liver. Focal lesions within the liver (arrows) enhancing on the arterial phase picture (A) and washing out on the delayed section image (B) with residual rim enhancement. These computed tomography findings are in maintaining with metastatic illness in a patient with recognized carcinoid tumor. A, Axial computed tomography picture shows a dilated distal small bowel phase (arrow) with concentric wall thickening with out inflicting any proximal bowel obstruction. B, Another axial picture by way of the stomach demonstrates multiple enlarged mesenteric lymph nodes (arrows). Coronal computed tomography (A), endoscopic (B), and endoscopic ultrasound (C) images show a well-defined, submucosal mass (arrows) in the second portion of the duodenum. Coronal T2-weighted (A) and contrast-enhanced axial T1-weighted (B) magnetic resonance photographs present a number of massive, peritoneal-based masses (arrows) and ascites. Nuclear Medicine A tagged purple blood cell scan is helpful in instances of acute gastrointestinal bleeding as a manifesting symptom of small bowel adenocarcinoma. Localization of the primary tumor to facilitate surgical procedure is better performed utilizing octreoscan in patients with carcinoid tumors. It is important to contemplate small bowel malignancies as a possible cause of those signs and to have a excessive stage of suspicion for catching them at an early stage. The medical differential analysis is huge and consists of ischemic, infectious, and inflammatory causes and different primary malignancies. Small bowel lymphoma and adenocarcinoma can manifest as small bowel obstruction or intussusception. The differential prognosis of lymphoma can include tuberculosis and inflammatory small bowel disease. The differential diagnosis consists of lymphoma, desmoid tumor, metastases, and mesenteric lymphadenopathy. Five-year survival charges range from 10% to 60%, with a median of approximately 30%. This take a look at is helpful in treatment planning and might predict the response to somatostatin analogs. Patients with positive octreoscan findings are treated with somatostatin analogs, which outcomes in control of signs (75%), stabilization of tumor development (71%), or tumor shrinkage (9%). Transarterial chemoembolization is the process of alternative for management of inoperable carcinoid liver metastases and reveals promising results with partial response in at least 50% of sufferers and a mortality fee of 5%. The treatment may vary from resection followed by chemotherapy for local tumor to only chemotherapy in advanced tumors. Radiation remedy is the treatment of choice for initially bulky tumor sites, remedy of residual illness after chemotherapy, or severe local problems. The most necessary factors that determine mode of therapy are small bowel tumor size and cell division price. Adenocarcinoma of the small bowel: review of the National Cancer Data Base, 1985-1995. Diagnostic highquality double-contrast barium enema examination is an art, requiring skillful maneuvering of the affected person and barium pool whereas optimally using fluoroscopy. Barium Enema Examination Single-contrast examination is most popular in immobile, aged, or incontinent patients.
Tanacetum Parthenium (Feverfew). Geriforte Syrup.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96896
Adhesions ridgecrest herbals anxiety free generic 100 caps geriforte syrup with amex, metastases herbs pool order 100 caps geriforte syrup visa, and radiation enteritis are thought-about in the differential diagnosis of small bowel obstruction in sufferers with identified malignancies herbs direct buy generic geriforte syrup 100 caps on-line. Abdominal tuberculosis may cause peritoneal thickening, mesenteric fat stranding, bowel wall thickening, and adenopathy mimicking metastatic disease. There is a big variability in the anticipated effectiveness of the remedy, in addition to in the prognosis of sufferers. Surgical Treatment Surgical treatment of secondary intestinal malignancies goals to relieve the intestinal obstruction and/or control the metastatic illness. An accurate preoperative understanding of the extent of the disease is essential for surgical planning. What the Referring Physician Needs to Know: Secondary Malignancies of the Small Bowel � Knowing if small bowel metastases are present changes the staging, and their presence may cause issues similar to intussusception, bleeding, or obstruction. Higher incidence of small bowel adenocarcinoma is also associated with adenomatous polyps, villous adenomas, familial adenomatous polyposis, hereditary nonpolyposis colorectal cancer, celiac sprue, cystic fibrosis, and peptic ulcer disease. Various predisposing elements have been postulated to be answerable for small bowel lymphoma. Carcinoid is the second most typical small bowel malignancy, representing roughly 25% of all primary small bowel tumors, and mostly impacts the ileum. In the past 30 years there has been an increase within the incidence of carcinoid tumors, with forty one. This remark might be as a outcome of the lowering price of appendectomies associated to the growing accuracy of diagnosing inflammatory appendicitis preoperatively. Synchronous or metachronous malignancies occur in 29% of sufferers with small intestinal carcinoids. Small bowel lymphoma is the third commonest small bowel malignancy, representing 10% to 15% of small bowel malignancies. It can involve any portion of the gastrointestinal tract and predominantly targets the lymphoid follicles. Mediterranean belly lymphoma is a variant related to immunoproliferative small intestinal disease and consists of diffuse lymphomatous infiltration of mucosa and submucosa in long segments of the small gut. There is a slight male predominance with bimodal age distribution, with peaks in those youthful than the age of 10 and older than the age of 50. Increased incidence of small bowel lymphoma was reported amongst sufferers with celiac disease. Clinical presentation consists of stomach ache in 66%, obstruction in 40%, and gross intestinal hemorrhage in 24% of sufferers. Patients with carcinoid tumor could be fully asymptomatic or may current with carcinoid syndrome (cutaneous flushing, sweating, bronchospasm, stomach ache, and diarrhea) in less than 10% of instances. Patients with small bowel lymphoma can present with persistent anemia, weight loss, fatigue, diarrhea, steatorrhea, or imprecise dull abdominal ache. Contraindications for the standard bowel preparation embrace bedridden sufferers, postoperative patients, patients with diabetes and hypothyroidism, and patients taking opiates. Before beginning the examine, compliance with the bowel preparation ought to be confirmed. Lubricant is applied on the external anal surface and the rectal catheter tip,9 and the catheter is gently inserted into the anal canal. The distal rectum is then drained by dropping the barium bag to the ground to avoid bubbles when air is insufflated. The patient is turned right facet down to fill the proximal transverse colon after which became the supine place to fill the posteriorly situated hepatic flexure. The enema tip can then be eliminated, providing bodily reduction to the affected person and permitting better analysis of the distal rectum. The enema tip could have to be left in place in patients expelling gasoline and who might have further air to visualize the terminal ileum. Technique Tips � Perform air insufflation solely after barium has passed the splenic flexure. Technique Tips � Sigmoid colon spot films are obtained before barium reaches the ascending colon. If barium refluxes via the ileocecal valve, the sigmoid colon could also be partly obscured. Some technical challenges throughout a double-contrast barium enema examination and believable options are summarized in Box 29-2. B, Postevacuation movie is necessary to detect lesions obscured by the barium pool. Allergic reactions may be noticed to barium, glucagon, or latex in gloves and rectal catheters. Barium impaction could cause delayed problems with various levels of constipation and/or abdominal pain. Venous intravasation could result from barium breaching the colonic mucosa and is a feared complication due to its high mortality price. A, the left hemicolon is diffusely mildly narrowed with loss of haustral markings (arrow). Deep "collar stud" ulcers (arrows) are current on a background of abnormal mucosa. Although the procedure is reimbursed by Medicare for colon screening, two large prospective scientific trials show the sensitivity of double-contrast barium enema examinations is roughly 50% for polyps measuring no much less than 10 mm in diameter. It is necessary to be well versed with regular appearances and variations on a double-contrast research. Luminal Distention When the lumen is optimally distended, the conventional mucosal folds are just effaced. Inadequate distention could conceal lesions, however overdistention can obscure lesions such as shallow ulcers. Mucosal Surface Variations the traditional mucosal floor usually has a clean, featureless appearance. En face, the mucosal surface fades from the white line of the contour to a clean, gray-white floor. A, Discrete aphthoid ulcers are seen on double-contrast barium enema surrounded by regular mucosa (arrows). B, Note extreme involvement of transverse colon with cobblestoning and ulceration (arrows). Lipoma Lipomas are the commonest colonic submucosal tumor and happen most regularly within the cecum and ascending colon. Benign pelvic masses similar to ovarian cysts and uterine fibroids produce smooth extrinsic mass impressions on the colonic wall. Colorectal Carcinoma the rectum and sigmoid areas are the most typical websites for carcinoma. Other manifestations include polypoid lesions, that are fungating and intraluminal plaque-like lesions with submucosal unfold and ulcerating tumors. Multiple barium-filled outpouchings (arrows) are noted in the sigmoid colon with spasm, mural thickening, and lack of distensibility of a focal phase of sigmoid colon. Artifacts Structures anterior or posterior to the bowel might project over the bowel and simulate lesions arising from the bowel. Flaking of barium produces an appearance suggestive of inflammatory bowel illness. Inadequate distention results in apposition of the anterior and posterior colonic walls, causing a "kissing" artifact that may resemble mass lesions. Note the graceful contour of the mass effect (arrow) without any signs of invasive illness. Annular constricting lesion seen as a short "apple core" phase (arrows) of narrowing with destruction of the mucosal sample in the transverse colon. Intravenous administration of distinction materials helps detect subtle bowel wall abnormalities. Delayed scans or decubitus views can clarify refined bowel findings, corresponding to colonic leak or perforation, pneumatosis, fistulas, and sinus tracts. Intravenous distinction material is crucial for enabling detection of subtle bowel wall abnormalities. The portal venous section normally is sufficient for Document t�l�charg� de ClinicalKey. Administration of intravenous contrast materials can also be essential for complete staging of colorectal most cancers.
Jaundice is an uncommon discovering (5% of cases) and outcomes from biliary compression by either the dominant tumor mass or mass effect of metastatic lymphadenopathy herbs mac and cheese generic 100 caps geriforte syrup with visa. The tumor also may manifest as signs related to metastatic dissemination to distant organs rajasthan herbals international discount geriforte syrup 100 caps with mastercard. On sectioning krishna herbals generic geriforte syrup 100 caps, lesions show a lobulated look, agency to exhausting consistency, and a attribute central fibrous scar with radiating septa. Areas of hemorrhage and necrosis can be seen within the tumor in fewer than half of circumstances. Besides common indicators of malignancy, such as biliary or vascular invasion and metastatic Document t�l�charg� de ClinicalKey. D, On corresponding picture in the course of the portal venous part, the tumor becomes isointense compared with the encircling liver. A central portion of the tumor that was of excessive signal intensity on T2-weighted imaging is noted as low sign intensity (arrow) on this sequence. Although these lesions have a central fibrous scar, the differential diagnosis relies on imaging findings of each the lesion and the scar. Larger lesions could manifest as a central, calcified scar, as on this case (arrow). Note coarse calcifications of the central scar (arrow) that characterize an indicator for this tumor. In Lencioni R, Cioni D, Bartolozzi C, editors: Focal liver lesions: detection, characterization, ablation, Berlin, 2005, Springer, pp 209�217. However, hemangiomas can be readily recognized primarily based on their typical enhancement sample (see Table 37-5). All sequence have reported long survival intervals after excision, with the longest postresection survival time of 21 years. The coincidence of hepatoblastoma with familial adenomatous polyposis and Beckwith-Wiedemann syndrome suggests a job within the pathogenesis of hepatoblastoma for chromosomes 5 and 11, respectively. Males are twice as commonly affected as females in early childhood, however tumor frequency is almost equal in older kids. Occasionally, paraneoplastic phenomena, corresponding to precocious puberty with genital enlargement, appearance of pubic hair, and a deepening voice could seem, owing to tumor overproduction of human chorionic gonadotropin. Two forms of hepatoblastoma have been described on histopathologic evaluation: the epithelial kind and the combined epithelial type. Because lesions are typically large, they may extend across the midline or all the means down to the pelvic brim. Areas of hemorrhage could be seen as intratumoral hyperintense foci on T1-weighted photographs, whereas calcification is depicted as signal void on T2-weighted images. Hepatoblastomas usually manifest as welldefined, strong, echogenic lesions on gray-scale ultrasonography. Occasionally, tumors might show a spoked-wheel appearance owing to prominent fibrous bands. In nearly all of cases, splenic involvement is also present at the time of detection. Occasionally, hepatic lymphoma may be incidentally discovered in asymptomatic sufferers. Pathology Primary and secondary hepatic lymphomas may manifest as both solitary or multifocal illness. Tumor dimension varies from a quantity of millimeters to a quantity of centimeters and is mostly bigger for solitary lesions. Misdiagnosis-as metastatic carcinoma, chronic hepatitis, or inflammatory pseudotumor-is widespread. Although lesions are usually isointense to hypointense relative to the liver on T1-weighted pictures, their appearance can range from low to reasonable hyperintensity on T2-weighted images and should reflect variations in tumor vascularity, size of extracellular area, and presence of necrosis and fibrosis. As a result of high cellularity, lymphomas usually present marked restricted diffusion. Elevated alpha-fetoprotein stage, however normal serum vanillylmandelic acid level, may present a clue for differentiating hepatoblastoma from neuroblastoma. Although prognosis of hepatoblastoma can be not often based mostly on imaging findings, a pattern of coarse and dense calcifications is suggestive of this neoplasm and permits differentiation with the fine granular calcifications of childish hemangioendothelioma. Despite the truth that 40% to 60% of hepatoblastomas are thought-about to be unresectable on the time of diagnosis, almost 85% of cases might turn out to be resectable after neoadjuvant chemotherapy. Surgery remains the mainstay within the treatment of hepatoblastoma, with prognosis immediately related to tumor stage. Liver transplantation has demonstrated promising outcomes and is at present carried out in patients with bigger lesions, including these requiring preoperative chemotherapy. Its frequent affiliation with hepatitis B and C virus an infection Document t�l�charg� de ClinicalKey. On gray-scale ultrasonography, primary hepatic lymphomas generally seem as well-defined, either anechoic or hypoechoic lesions that mimic easy hepatic cysts, except for the absence of increased through-transmission. A portal venous branch (white arrowhead) extending by way of the lesion is barely seen. Although an infiltrative appearance (arrows) is generally considered a worrisome sign, differential analysis among each malignant and benign liver lesions is regularly challenging solely based mostly on imaging findings. Primary lymphoma exhibits a wonderful response rate associated with the use of mixture chemotherapy alone. Surgery alone has been advocated for those sufferers with small solitary hepatic lesions, although its efficacy is regularly restricted by early extrahepatic recurrence. The most common major sites for liver metastases embrace the gastrointestinal tract, pancreas, gallbladder, breast, lung, eye, and carcinoids. In superior phases, indicators and symptoms are referred to liver involvement and embrace hepatomegaly, anorexia, weight loss, and proper higher quadrant belly pain (30% to 40%). The cause for this distribution is unclear, although attainable reasons could be the greater total mass of the right lobe compared with the left lobe and underlying differences in laminar portal vein circulate patterns, which can information the distribution of metastatic cells. Pathology Liver metastases sometimes manifest as multiple irregular nodules, with a variable size starting from a few millimeters to several centimeters. Central areas of avascular necrosis can be incessantly seen on the heart of the lesions. After chemotherapy, metastases may demonstrate an umbilicated look owing to scarring and retraction. On histologic examination, metastases closely resemble the appearance of main tumor. By taking advantage of histochemical and immunohistochemical stains, skilled pathologists often can recommend the primary website when unknown. Prevalence and Epidemiology Metastases are by far the most common malignant neoplasm of the liver. In the United States, it has been estimated that up to Document t�l�charg� de ClinicalKey. Imaging Clinical signs and symptoms referable to the liver are usually related to far advanced tumor phases as nicely as in depth liver involvement. Occasionally, intratumoral calcifications could be seen in mucinous adenocarcinoma metastases. In the setting of diffuse fatty liver disease, metastases could seem hyperintense on opposed-phase T1-weighted images owing to substantial signal drop of the encompassing hepatic parenchyma. On diffusion weighted images, metastases present restricted diffusion with uniform, variegated, or peripheral hyperintensity at high b-values. Based on the sturdy, homogeneous hypervascularity (arrow, B) during the hepatic arterial section and on the central space of hypoattenuation simulating a central scar (long thin arrow, B), the lesion enters in differential diagnosis with focal nodular hyperplasia. However, robust hypoattenuation (arrowhead) on noncontrast picture (A), washout through the portal venous phase (C), and the historical past of a identified main neoplasm all favor metastatic illness. Transverse diffusion weighted images reveal two small metastases (arrow), which present hyperintensity at b zero sec/mm2, and remain hyperintense at b 150 sec/ mm2 (B) and b 600 sec/mm2 (C), indicating restricted diffusion. Also observe a small cyst (arrowhead) with sign intensity lower at b 600 sec/mm2 in contrast with that at b 0, and marked hypointensity on hepatobiliary section. Although ultrasonography is generally associated with a poor diagnostic efficiency, microbubble distinction agents have shown the potential to enhance the accuracy of ultrasonography for the detection of liver metastases. Intraoperative ultrasonography is a crucial adjunct during surgical procedure to accurately outline the anatomic relationship between tumors and major vascular and biliary buildings and for detection of beforehand unsuspected liver lesions. Although the peripheral rim enhancement of hypovascular metastases with centripetal development can be mistaken for cavernous hemangiomas, lesion washout on delayed images, delicate hyperintensity on T2-weighted pictures, and, lower apparent diffusion coefficient values on diffusion weighted pictures are all indicative findings of liver metastases.
Signal void may be seen throughout the cystic areas when intracystic calculi are current herbs menopause geriforte syrup 100 caps order on-line. On gadolinium administration herbals incense generic 100 caps geriforte syrup visa, the focal mass shows enhancement whereas the cystic areas are nonenhancing aasha herbals - geriforte syrup 100 caps otc. A "diamond ring" appearance may be seen on transverse sections due to the ringlike distribution of the hyperintense cystic structures around the gallbladder wall on T2-weighted photographs. Occasionally, this artifact may be mistaken for air inside the gallbladder lumen or wall (emphysematous cholecystitis), which might have an identical look. Whereas the dirty shadow of air is more linear in configuration, the reverberation artifacts of adenomyoma are V shaped. The three variants of adenomyomatous hyperplasia are localized (or fundal), segmental, and diffuse. A to C, Axial contrast-enhanced computed tomography images of the stomach show focal wall thickening of the gallbladder at the fundus (arrows). The small cystic areas of water attenuation are greatest seen in B and C throughout the focal wall thickening and characterize the Rokitansky-Aschoff sinuses crammed with bile. Classic Signs: Adenomyoma � A focal wall thickening or mass with intramural cystic areas is seen. Adenocarcinomas normally end in localized thickening of the gallbladder wall after causing it to bulge into the lumen. Infiltrating carcinomas with submucosal unfold can appear as focal wall thickening with nodularity and induration of the gallbladder wall. Computed Tomography Focal wall thickening seen in gallbladder carcinoma could be confused with appearances of more frequent inflammatory circumstances of the gallbladder. However, the presence of pronounced wall thickening (>1 cm) with related mucosal irregularity suggests malignancy. These polypoid lots improve homogenously and the adjacent gallbladder wall exhibits thickening, which enhances in the venous phase. However, if signs do occur, the presentation is much like that of some other gallbladder disease. Axial contrast-enhanced (A) and coronal reformatted (B) computed tomography images of the abdomen present a focal gallbladder carcinoma (arrows) adjoining to the gallbladder fossa invading into the adjoining hepatic parenchyma and with related extensive hepatic metastases. Axial contrast-enhanced (A) and coronal reformatted (B) computed tomography pictures present the metastatic focus (arrows) appearing as a focal enhancing mass in the fundus protruding into the gallbladder lumen. The tumor seems hypointense on T1-weighted images and hyperintense on T2-weighted photographs in contrast with the liver parenchyma. Illdefined early enhancement is typical of gallbladder carcinoma on dynamic imaging. Malignant polypoid lesions larger than 1 cm show early and extended enhancement, whereas benign lesions show early enhancement with subsequent washout. Ultrasonography Focal gallbladder wall thickening or focal polypoid mass is seen with overlying mucosal irregularity and heterogenous echotexture. It is possible to differentiate gallbladder carcinoma from sludge, nonshadowing calculi, and blood clot based mostly on movement in actual time. Gallbladder Classic Signs: Gallbladder Carcinoma � Focal gallbladder wall thickening occurs with surface nodularity and mucosal irregularity. Gallbladder metastases can manifest as polypoid lesions or infiltrative wall thickening. The ultrasound appearance of melanoma metastases is that of single or multiple hyperechoic plenty larger than 1 cm in diameter and hooked up to the gallbladder wall. What the Referring Physician Needs to Know Gallbladder Adenoma � Gallbladder adenomas are incidental findings on imaging. Adenomyoma � Adenomyomatosis of the gallbladder is an incidental finding on imaging. Gallbladder Carcinoma � Focal gallbladder wall thickening or a focal mass is amongst the frequent manifestations of gallbladder carcinoma. Cholesterol Polyps � these asymptomatic incidental lesions account for 50% of polypoid lesions of the gallbladder. Adenomyoma � Adenomyomatosis is an acquired, benign, and degenerative situation of the gallbladder mostly seen in adults. Gallbladder Carcinoma � the assorted imaging appearances of gallbladder carcinoma embrace focal or diffuse wall thickening, polypoidal intraluminal lesion, or an infiltrating mass replacing the gallbladder. Wada K, Tanaka M, Yamaguchi K, et al: Carcinoma and polyps of the gallbladder related to Peutz-Jeghers syndrome. Turrini R, Lanzani G, Salmi A: [Gallbladder adenoma with focal adenocarcinoma: a case report]. Terzi C, Sokmen S, Seckin S, et al: Polypoid lesions of the gallbladder: report of one hundred instances with particular reference to operative indications. Kaido T, Kano M, Suzaki S, et al: Large ldl cholesterol polyp of the gallbladder mimicking Document t�l�charg� de ClinicalKey. Takayama Y, Asayama Y, Yoshimitsu K, et al: Metastatic melanoma of the gallbladder. Modern useful strategies are noninvasive and might allow earlier and improved illness characterization resulting in acceptable and well timed affected person care. Although highly delicate within the analysis of the gallbladder, ultrasound is restricted in assessment of the extrahepatic biliary tree and intrahepatic bile ducts within the absence of biliary dilatation. However, practical evaluation of the biliary tree is predicated on evaluation of morphologic changes such as biliary duct dilatation, stricture, or filling defects. Oral cholecystography or cholescintigraphy permit noninvasive practical evaluation of the gallbladder and the biliary tree (see later discussion). Both the latter methods require administration of contrast agents, which are eradicated via the biliary ducts, and have the potential to provide comprehensive analysis of both the anatomy and function of the gallbladder and biliary tree. Exclusive distribution to the hepatocellular compartment can be obtained using distinction agents that, when injected by gradual infusion, accumulate throughout the hepatocytes and trigger an increase in the proton leisure price. As a results of its 5 unpaired electrons, manganese is moderately paramagnetic, resulting in excessive signal depth on T1-weighted photographs. After intravenous injection, mangafodipir trisodium is taken up by functioning hepatocytes through vitamin B6 receptors. Extrahepatic uptake is observed when a few of the manganese dissociates from its ligand throughout the blood circulation. The free manganese is then obtainable for uptake into parenchymal cells, significantly those of the liver, pancreas, kidneys, and adrenals, during which metabolism of this steel takes place. In Europe, mangafodipir trisodium is infused slowly (2 to 3 mL/min over a 10- to 20-minute period) at a dosage of 5-10 mol/kg, whereas in the United States a quicker injection (~1 minute) is employed. The maximum tissue enhancement is observed at the finish of the infusion after roughly 20 minutes and lasts for around four hours. Several studies have shown improved lesion detection on pictures obtained after infusion of mangafodipir trisodium. Uptake of mangafodipir trisodium, and subsequently enhancement, by both benign and malignant hepatic neoplasms of hepatocellular origin limits their accurate differentiation and therefore represents a significant shortcoming of this agent. This excretion reflects the performance of the hepatocytes and makes the bile brilliant on T1-weighted sequences. The excessive sign depth of the biliary system during excretion of the contrast agent produces wonderful distinction with the liver parenchyma and hepatic vessels in the background. Spin echo T2-weighted magnetic resonance image (A) exhibits a hyperintense lesion with central necrotic modifications. Gradient recalled echo T1-weighted images earlier than (B) and after (C) administration of mangafodipir trisodium. After administration of the contrast agent there is an increase of the distinction ratio owing to the shortage of uptake of the agent by the lesion. After administration of the distinction agent the lesion is hyperintense with a decrease of the distinction ratio owing to uptake of the agent by the lesion. Other distinction brokers show mixed perfusion and hepatocyte-selective properties. Such compounds distribute initially to the vascular-interstitial compartment in a way analogous to that of the traditional, extracellular contrast agents. Thereafter, a fraction of the injected dose is taken up into the hepatocytes, causing an increase of the signal intensity of the hepatic tissue. It was approved to be used within the United States in December 2004 and has been utilized in Europe for several years. The maximum improve of liver parenchyma signal intensity is noticed roughly 20 minutes after injection and lasts for roughly 2 hours. D to H, On magnetic resonance imaging the lesion is isointense each on T2-weighted (D) and unenhanced T1-weighted gradient recalled echo (E) pictures.






