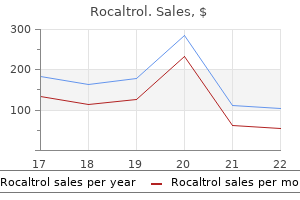
Rocaltrol
Rocaltrol
Rocaltrol dosages: 0.25 mcg
Rocaltrol packs: 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Massive intravascular haemolysis throughout Clostridium perfringens sepsis of hepatic origin medications 101 generic rocaltrol 0.25 mcg line. Massive intravascular hemolysis from Clostricium perfringens septicemia: a review 25 medications to know for nclex buy discount rocaltrol 0.25 mcg online. Brown recluse spider (Loxosceles reclusa) envenomation resulting in treatment pink eye rocaltrol 0.25 mcg generic on line acute hemolytic anemia in six adolescents. Anemia of thermal harm: combined acute blood loss anemia and anemia of crucial illness. Compare and distinction mechanisms of immune hemolysis mediated by immunoglobulin M (IgM) and IgG antibodies. Describe two forms of hemolytic transfusion reactions, the same old immunoglobulin class involved, typical website of hemolysis, and necessary laboratory findings. Compare and contrast the pathophysiology of immune hemolysis brought on by drug-dependent and drugindependent antibodies, together with associated laboratory findings. Given a patient history and results of an entire blood count, peripheral blood movie examination, pertinent biochemical exams on serum and urine, and the direct and oblique antiglobulin tests, decide the kind of immune hemolysis. There was no significant medical history and the affected person was not taking any drugs. Occasional schistocytes and neutrophilia with a slight left shift have been additionally noticed on the blood film (not shown in figure). The patient was continued on prednisone for 4 months with slowly reducing ranges of the drug. He also obtained bisphosphonates, vitamin D, and calcium to stop osteoporosis, an opposed effect of prednisone. Describe the immune mechanism that triggered the spherocytosis, and clarify why spherocytes have a shortened life span. The degree of anemia varies from asymptomatic and mild to extreme and life threatening. Immune hemolytic anemias could also be categorised into the next teams: autoimmune hemolytic anemia, alloimmune hemolytic anemia, and drug-induced immune hemolytic anemia (Box 23. Two courses or isotypes of antibodies involved in most immune hemolytic anemias are immunoglobulin G (IgG) and M (IgM). IgG is a monomer in a Y-like structure with two equivalent heavy chains (g H chains) and two identical gentle chains (either k or l) connected by disulfide bonds. Major proteins of the classical complement pathway are designated C1 through C9, and their elements or fragments are designated with lowercase suffixes. In these circumstances, complement activation proceeds from C1 to C9 and results in fast intravascular hemolysis. If hemolysis is predominantly intravascular, or extravascular hemolysis is severe, the haptoglobin level will be reasonably to severely decreased, plasma hemoglobin might be elevated, and the affected person may have hemoglobinuria or even hemosiderinuria (in cases of persistent hemolysis) (Chapter 20). Leukocytosis and thrombocytosis might occur along with increased erythroid proliferation in bone marrow. The complicated activates C2 and C4 to kind the C4bC2a complicated (C3 convertase) on the membrane. C3b also can kind the complicated C4bC2aC3b (C5 convertase), which converts C5 to C5b on the membrane. C5b varieties the membrane attack advanced, C5bC6C7C8C9, which inserts into the bilipid layer, causing lysis. The anti-IgG produces agglutination by binding to the Fc domain of immunoglobulin G (IgG) antibodies which might be sure to antigens on the red blood cell membranes. Similarly, the anti-C3d/C3b produces agglutination by binding to the respective complement components if present on the purple blood cell membranes (reaction not shown). Cold Agglutinin Disease Cold agglutinins are autoantibodies of the IgM class that react optimally at 4� C and are commonly present in healthy people. These cold agglutinins are polyclonal IgM, with a traditional distribution of k and l mild chains. Most sufferers have a gentle anemia with a hemoglobin outcome starting from 9 to 12 g/dL, however others can develop life-threatening anemia with hemoglobin levels falling to lower than 5 g/dL, especially after exposure to cold temperatures. Blood specimens from patients with chilly agglutinins have to be warmed to 37� C for no less than quarter-hour earlier than complete blood count evaluation by automated blood cell analyzers. The patient control tube is kept at 37� C for each incubations (a total of 60 minutes). A positive check result for anti-P is indicated by hemolysis within the affected person take a look at specimen incubated first at 4� C and then at 37� C and no hemolysis within the patient control specimen kept at 37� C. If not, a brand new specimen is collected and maintained at 37� C for the whole time before testing. To avoid agglutination on a peripheral blood film, the slide can be warmed to 37� C earlier than the appliance of blood. During transfusion, the affected person is saved heat, small amounts of blood are given whereas the patient is noticed for signs of a hemolytic transfusion response, and a blood hotter is used to reduce in vivo reactivity of the chilly autoantibody. Because anti-P autoantibody reacts solely at lower temperatures and P antigennegative blood is very rare, P-positive blood can be transfused. The illness course seems to be continual, with intermittent episodes of severe anemia. The offending antibody in the recipient could also be IgM or IgG, complement could additionally be partially or totally activated or not activated at all, and hemolysis could also be intravascular or extravascular, relying on the traits of the antibody. There is rapid, complementmediated intravascular hemolysis and activation of the coagulation system. The second publicity to the antigen results in an increase in titer (anamnestic response). The antibody is normally IgG, is reactive at 37� C, and will or may not be succesful of partially or totally activate complement. There is erythroid hyperplasia in the fetal bone marrow and extramedullary erythropoiesis within the fetal spleen, liver, kidneys, and adrenal glands. If anemia is extreme in utero, it can result in generalized edema, ascites, and a condition referred to as hydrops fetalis, which is deadly if untreated. Certain antibodies could additionally be ignored if their corresponding antigens are poorly developed at start, corresponding to anti-I, anti-P1, anti-Lea and -Leb. Mothers with initial constructive antibody screens are retested with an antibody display screen every month till 28 weeks, then each 2 weeks thereafter; antibody titers are reported from each specimen. Survival charges of fetuses receiving transfusions are 85% to 90%; the chance of untimely death from these procedures varies from 1% to 3%. The patient produces an antidrug immunoglobulin G (IgG) antibody that binds to the drug. The patient produces an IgG and/or IgM (not shown) antibody that binds to the advanced, causing complement activation and acute intravascular hemolysis. Hemolysis is extravascular and is mediated by macrophages predominantly in the spleen. Several authors have suggested that each one drug-induced immune hemolysis is defined by a single mechanism, known as the unifying theory. The antibodies activate complement and set off acute intravascular hemolysis that will progress to renal failure. Hemolysis is extravascular, mediated by macrophages predominantly in the spleen, often with a gradual onset of anemia. Anemia varies from delicate to extreme, and characteristic morphologic features on the peripheral blood film are polychromasia and spherocytes. The most necessary finding within the diagnostic investigation of a suspected autoimmune hemolytic anemia is: a. It is as a end result of of an anamnestic response after repeat publicity to a blood group antigen d. A 63-year-old man is being evaluated due to a decrease in hemoglobin of 5 g/dL after a second cycle of fludarabine for remedy of persistent lymphocytic leukemia. Classification and therapeutic approaches in autoimmune hemolytic anemia: an update. Treatment options for main autoimmune hemolytic anemia: a brief comprehensive evaluate.
The platelet depend decreases with rising age medicine 750 dollars 0.25 mcg rocaltrol order, such that after sixty five years of age treatment concussion generic rocaltrol 0.25 mcg on line, platelet counts of 122 to 350 3 109/L and one hundred forty to 379 3 109/L are seen in women and men medicine names 0.25 mcg rocaltrol cheap with mastercard, respectively. This depend represents solely two thirds of complete physique platelets; the remaining one third is sequestered throughout the spleen. Sequestered platelets are instantly available in times of demand- for example, in acute inflammation or after an damage, after major surgery, or throughout plateletpheresis. In hypersplenism or splenomegaly, elevated sequestration might cause a relative thrombocytopenia. Reticulated platelets carry free ribosomes and fragments of tough endoplasmic reticulum, analogous to purple blood cell reticulocytes, which triggers hypothesis that they arise from early and speedy proplatelet extension and launch. Reticulated platelets are probably prothrombotic and could additionally be related to elevated threat of cardiovascular disease. The stress platelet may seem in blood circulation in compensation for thrombocytopenia. Reticulated platelets carry free ribosomes and fragments of rough endoplasmic reticulum, detectable in move cytometry using nucleic acid dyes. Their ultrastructure has been studied using scanning and transmission electron microscopy, move cytometry, and molecular sequencing. The platelet possesses a normal biologic membrane composed of a phospholipid bilayer with polar head teams oriented toward the aqueous blood plasma (neutral phospholipids) and platelet cytoplasm (charged phospholipids) and nonpolar fatty acid tails that orient toward the middle. The phospholipid spine is interspersed with esterified ldl cholesterol that maintains membrane integrity and performance. A collection of transmembranous proteins communicate with microfilaments (shown here), G-proteins, and enzymes. The transmembranous proteins support carbohydrate side chains (receptors) that extend into the plasma. The phospholipids form a bilayer with their polar heads oriented toward aqueous environments-toward the blood plasma externally and the cytoplasm internally. Their fatty acid chains, esterified to carbons 1 and 2 of the phospholipid triglyceride spine, orient toward each other, perpendicular to the aircraft of the membrane, to kind a hydrophobic barrier sandwiched inside the hydrophilic layers. The neutral phospholipids phosphatidylcholine and sphingomyelin predominate within the outer blood plasma layer; the anionic or polar phospholipids phosphatidylinositol, phosphatidylethanolamine, and phosphatidylserine predominate within the internal, cytoplasmic layer. During platelet activation these phospholipids, particularly phosphatidylinositol, support platelet activation by supplying arachidonic acid, an unsaturated fatty acid that becomes converted to the eicosanoids, including the potent thromboxane A2 (detailed later in this chapter). Esterified cholesterol strikes freely throughout the hydrophobic inner layer, exchanging with unesterified ldl cholesterol from the encompassing plasma. Cholesterol stabilizes the membrane, maintains fluidity, and helps management the transmembranous passage of supplies through the selectively permeable plasma membrane. Anchored throughout the membrane are glycoproteins and proteoglycans that help surface glycosaminoglycans, oligosaccharides, glycolipids, and important plasma surface-oriented glycosylated receptors that respond to mobile and humoral stimuli, called ligands or agonists, transmitting their stimulus by way of the membrane to activation organelles internal to the platelet. The platelet membrane surface, referred to as the glycocalyx, additionally absorbs albumin, fibrinogen, and other plasma proteins, in many cases transporting them to inner storage organelles using a process referred to as endocytosis. At 20 to 30 nm, the platelet glycocalyx is thicker than the analogous floor layer of leukocytes or erythrocytes. The platelet carries its practical setting with it, meanwhile sustaining a adverse floor charge that repels other Microtubules Dense body platelets, different blood cells, and the endothelial cells that line the blood vessels. The circumferential microtubules parallel the airplane of the outer surface of the platelet and reside just inside, though not touching, the plasma membrane. There are 8 to 20 tubules composed of a number of subunits of tubulin that disassemble at refrigerator temperature or when platelets are handled with colchicine. When microtubules disassemble within the chilly, platelets turn into round, but on warming to 37� C, they recover their original disc shape. In the narrow area between the microtubules and the membrane lies a thick meshwork of microfilaments composed of actin. Actin is contractile in platelets (as in muscle) and anchors the plasma membrane glycoproteins and proteoglycans. Actin also is present all through the platelet cytoplasm, constituting 20% to 30% of platelet protein. In the resting platelet, actin is globular and amorphous, however because the cytoplasmic calcium concentration rises, actin becomes filamentous and contractile. The cytoplasm additionally incorporates intermediate filaments, ropelike polymers eight to 12 nm in diameter, of desmin and vimentin. The intermediate filaments join with actin and the tubules, maintaining the platelet form. Microtubules, actin microfilaments, and intermediate microfilaments control platelet form change, extension of pseudopods, and secretion of granule contents. The a-granules are filled with proteins, some endocytosed, some synthesized within the megakaryocyte and stored in platelets (Table 10. Their contents move to the close by microenvironment, the place they take part in platelet adhesion and aggregation and support plasma coagulation. These granules seem later than a-granules in megakaryocyte differentiation and stain black (opaque) when treated with osmium in transmission electron microscopy. Small molecules are most likely endocytosed and are saved in the dense granules; these are listed in Table 10. The contents of lysosomes probably digest vessel wall matrix parts during in vivo aggregation and can also digest autophagic particles. Several integrins bind collagen, enabling the platelet to adhere to the injured blood vessel lining. Likewise, a5b1and a6b1 bind the adhesive endothelial cell proteins laminin and fibronectin, which further promotes platelet adhesion. Thrombin cleavage of either of these two receptors activates the platelet via G-proteins that in turn activate no much less than two internal physiologic pathways. Epinephrine binds a2-adrenergic websites that couple to G-proteins and open membrane calcium channels. P-selectin quantification by circulate cytometry is a typical means for measuring in vivo platelet activation. Shear forces range from 500 s21 in venules and veins to 5000 s21 in arterioles and capillaries and up to forty,000 s21 in stenosed (hardened) arteries. This is a reversible binding course of that "tethers" thereby decelerating the forward motion of the platelet. P-selectin from the a-granule membranes strikes to the surface membrane to promote binding of platelets with leukocytes. On additional activation, in conjunction with aggregation, platelets change in form from discoid to spherical and prolong pseudopods. This allows platelets to cover extra floor area and it enhances platelet binding to different platelets and overseas surfaces. Membrane phospholipid asymmetry is lost, with the more polar molecules, especially phosphatidylserine, flipping to the outer layer. As platelet aggregation continues, membrane integrity is misplaced, and a syncytium or huge clump of platelets forms because the platelets exhaust inner energy sources. By presenting polar phospholipids on their membrane surfaces, platelets present a localized cellular milieu that helps coagulation. The formation of both complexes is supported by ionic calcium secreted by the dense granules. Generation of Platelet Microparticles Microparticles are membrane-derived vesicles that kind in response to an activating stimulus that will increase the platelet intracellular focus of calcium. Elevated levels of intracellular calcium end in an inhibition of the enzymes liable for sustaining the uneven distribution of phospholipids in the plasma membrane and an activation of intracellular calpain, which cleaves the platelet cytoskeleton. Together, these results lead to the outward blebbing of the plasma membrane and the formation of platelet microparticles. Platelet microparticles, believed to be essentially the most ample microparticles within the circulation, are fashioned after publicity of platelets to robust agonists or shear stress. Fibrin and red blood cells deposit round and throughout the platelet syncytium to type a bulky "pink clot. Intermediate filaments additionally contract, moving the circumferential microtubules inward compressing the granules. As such, microparticles have been found to modulate irritation, oxidative stress, angiogenesis, and thrombosis.
Application of third-dimensional computed tomographic picture steerage to watchman implantation and influence on early operator studying curve: single-center expertise symptoms bronchitis generic rocaltrol 0.25 mcg amex. Left atrial appendage closure underneath intracardiac echocardiographic guidance: feasibility and comparability with transesophageal echocardiography symptoms after miscarriage 0.25 mcg rocaltrol generic with mastercard. Intracardiac versus transesophageal echocardiography for left atrial appendage occlusion with watchman treatment programs trusted rocaltrol 0.25 mcg. Initial expertise with a novel percutaneous left atrial appendage exclusion system in sufferers with atrial fibrillation, increased stroke danger, and contraindications to anticoagulation. Early security and efficacy of percutaneous left atrial appendage suture ligation: outcomes from the U. Multicenter research on acute and long-term security and efficacy of percutaneous left atrial appendage closure using an epicardial suture snaring gadget. Initial experience with post Lariat left atrial appendage leak closure with Amplatzer septal occluder system and repeat Lariat software. Ischemic stroke in sufferers with atrial fibrillation: effect of aspirin according to stroke mechanism. Currently, the transvenous or transseptal strategy utilizing the Inoue balloon is essentially predominant. Transseptal Approach the transvenous, or antegrade, strategy is carried out through the femoral vein. Transseptal catheterization is the essential first step of the process, often carried out underneath fluoroscopic guidance and steady strain monitoring. Intracardiac echocardiography could also be used with out further operators or general anesthesia, though the value of the device significantly limits its use. After transseptal catheterization, a stiff guidewire is introduced into the left atrium. The femoral entry site and the atrial septum are dilated with a rigid dilator (14 Fr), and the balloon is launched into the left atrium. Inoue recommended using a stepwise dilation method under echocardiographic steerage. First, the distal portion is inflated with 1 or 2 mL of diluted distinction; it acts as a floating balloon catheter when crossing the mitral valve. Second, the distal part is further inflated, and the balloon is pulled again into the mitral orifice. The first inflation is carried out 4 mm below the maximal balloon size, and the balloon measurement is elevated in 1-mm increments. Other Techniques the double-balloon approach has been described extensively and long-term results are comparable to these of the Inoue balloon. Echocardiography permits detection of early problems corresponding to pericardial hemorrhage and severe mitral regurgitation. Inoue Technique the Inoue method was the primary to be described, and intensive experience has been acquired by many teams worldwide. The Inoue balloon, composed of nylon and rubber micromesh, is selfpositioning and pressure extensible. The balloon has three distinct parts, every with a selected elasticity, enabling the components to be inflated sequentially. This sequence permits Monitoring the Procedure Planimetry using two-dimensional echocardiography is the reference methodology. The commissural opening is often assessed in the parasternal short-axis view (Videos 51. When obtainable, real-time threedimensional echocardiography is the most correct method for assessing the diploma of commissural opening using short-axis views (Video fifty one. After the process, probably the most accurate analysis of the valve space is achieved by echocardiography. Color Doppler flow is used to assess the diploma of regurgitation and interatrial shunting. It additionally decreases the depth of spontaneous echocardiographic contrast in the left atrium. Pericardial hemorrhage may be associated to transseptal catheterization or to apex perforation by guidewires or the balloon and has become unusual with the Inoue technique. It may be caused by gasoline immediately after balloon rupture, by fibrinothrombotic materials, or often, by calcium accumulation. Severe mitral regurgitation is rare, between 2% and 19%, was approximately 5% in large series, and stays largely unpredictable for a given patient. It may be brought on by extreme commissural splitting or hardly ever by rupture of a papillary muscle. Development of extreme regurgitation depends more on the distribution of morphologic adjustments than on their severity. In most instances, valve substitute is important and is more carefully associated to the extent of valve illness than to the tear itself. Urgent surgery (within 24 hours) is seldom wanted, mainly due to huge hemopericardium or severe and poorly tolerated mitral regurgitation. The degree of mitral regurgitation stays steady or barely decreases throughout follow-up. Vitamin K blockers ought to be used due to the lack of knowledge with direct oral anticoagulants. Because of the small however particular danger inherent within the approach, the indications for intervention are limited to really symptomatic sufferers with extreme mitral stenosis. Contraindications to transseptal catheterization embrace primarily suspected left atrial thrombosis, severe hemorrhagic disorder, and extreme cardiothoracic deformity. For older sufferers, valvuloplasty leads to a average however important improvement in valve function at a suitable threat, though subsequent useful deterioration is common. During pregnancy, surgical procedure beneath cardiopulmonary bypass carries a considerable risk of fetal mortality and morbidity. For patients with a previous surgical commissurotomy, reoperation is related to a better danger of morbidity and mortality and requires valve substitute generally. In instances of mixed mitral stenosis and severe aortic illness, surgical procedure is indicated in the absence of contraindications. Combined severe tricuspid stenosis and tricuspid regurgitation with clinical indicators of heart failure is a sign for surgical procedure on both valves. Most widely used scores have a prognostic value on immediate and late outcomes but should be analyzed at the facet of other affected person traits. Twenty yr follow-up after successful percutaneous balloon mitral valvuloplasty in a big contemporary collection of sufferers with mitral stenosis. The echo score revisited: influence of incorporating commissural morphology and leaflet displacement to the prediction of end result for patients present process percutaneous mitral valvuloplasty. Valve replacement is a radical therapy when valve anatomy is impaired, however is associated with larger operative mortality and prosthesis-related complications, which are of specific significance in young patients. Current opinion is that open surgical procedure could be considered the treatment of alternative for sufferers with bicommissural or heavy calcification. Conversely, information recommend that balloon valvuloplasty can be tried as a first strategy in sufferers with somewhat unfavorable anatomy, particularly if their scientific standing argues in favor of it. It reproduces an efficient surgical process, with a much less invasive approach, and its long-term efficacy has been demonstrated. In developed countries, the issues are completely different as a end result of most candidates are older and have somewhat much less favorable anatomy. High risk of hemodynamic decompensation: systolic pulmonary strain >50 mm Hg at rest, need for main noncardiac surgical procedure, need for pregnancy. Anatomical characteristics: echocardiographic rating >8, Cormier score three (calcification of mitral valve of any extent as assessed by fluoroscopy), very small mitral valve space, extreme tricuspid regurgitation. Predicting success and long-term outcomes of percutaneous mitral valvuloplasty: a multifactorial rating. Percutaneous balloon versus surgical closed and open mitral commissurotomy: seven-year follow-up outcomes of a randomized trial. Late end result of percutaneous mitral commissurotomy: randomized comparison of Inoue versus double-balloon approach. Percutaneous transvenous mitral commissurotomy: immediate and long-term follow-up outcomes. Retrograde nontransseptal balloon mitral valvuloplasty: quick outcomes and intermediate long-term consequence in 441 cases-a multicenter experience.
Describe the characteristic peripheral blood and bone marrow features in aplastic anemia medicine cabinet buy 0.25 mcg rocaltrol mastercard. Classify aplastic anemia as nonsevere medications you cant take with grapefruit rocaltrol 0.25 mcg discount with visa, severe medications ending in pam discount 0.25 mcg rocaltrol overnight delivery, or very severe based mostly on laboratory tests. Discuss remedy modalities for acquired aplastic anemia and inherited bone marrow failure syndromes and the patients for whom every is most applicable. Differentiate amongst causes of pancytopenia based on laboratory tests and scientific findings. Compare and distinction the pathophysiology, medical picture, and laboratory findings in Fanconi anemia, dyskeratosis congenita, Shwachman-Bodian-Diamond syndrome, transient erythroblastopenia of childhood, Diamond-Blackfan anemia, and congenital dyserythropoietic anemia. Describe the mechanisms inflicting cytopenia in myelophthisic anemia and anemia of continual kidney disease. She was referred to a gastroenterologist, who recognized her with autoimmune hepatitis. However, over the following several months, she seen rising fatigue and bruising. Physical examination revealed pallor and scattered ecchymoses with petechiae on her chest and shoulders with no other abnormalities. Bone marrow aspirate revealed gentle dyserythropoiesis however normal myelopoiesis and megakaryopoiesis. A bone marrow biopsy specimen was moderately hypocellular (15%) with a reduction in all three cell traces. Cytogenetic testing revealed a traditional karyotype, and outcomes of circulate Continued *The authors lengthen appreciation to Elaine M. What time period is used to describe a decrease in all cell traces within the peripheral blood How would a rise in both reticulin or blasts alter the preliminary prognosis The pathophysiology of bone marrow failure contains (1) destruction of hematopoietic stem cells as a outcome of damage by medicine, chemical compounds, radiation, viruses, or autoimmune mechanisms; (2) untimely senescence and apoptosis of hematopoietic stem cells on account of genetic mutations; (3) ineffective hematopoiesis caused by stem cell mutations or vitamin B12 or folate deficiency; (4) disruption of the bone marrow microenvironment that helps hematopoiesis; (5) decreased manufacturing of hematopoietic growth elements or related hormones; and (6) lack of normal hematopoietic tissue as a outcome of infiltration of the marrow house with irregular cells. Clinical consequences of bone marrow failure range, relying on the extent and length of the cytopenias. Some sufferers might initially be asymptomatic, and their cytopenia could also be detected during a routine blood examination. Sustained neutropenia will increase the danger of lifethreatening bacterial or fungal infections. This article focuses on aplastic anemia, a bone marrow failure syndrome ensuing from broken or defective stem cells (mechanisms 1 and a pair of listed earlier). Bone marrow failure ensuing from different mechanisms might present equally to aplastic anemia, and differentiation is discussed later. Because there are heaps of mechanisms involved within the various bone marrow failure syndromes, accurate analysis is crucial to ensure appropriate treatment. Approximately 70% of all aplastic anemia instances are idiopathic, whereas 10% to 15% are secondary. Patients may initially current with macrocytic or normocytic anemia and reticulocytopenia. Pancytopenia could develop slowly or progress at a rapid rate, with full cessation of hematopoiesis. Incidence In North America and Europe the annual incidence is approximately 1 in 500,000. In 1888 Ehrlich supplied the first case report of aplastic anemia involving a affected person with extreme anemia, neutropenia, and a hypocellular marrow on postmortem examination. Secondary aplastic anemia is related to publicity to certain drugs, chemicals, radiation, or infections. Cytotoxic medicine, radiation, and benzenes are answerable for 10% of secondary aplastic anemia instances and suppress the bone marrow in a predictable, dose-dependent method. Alternatively, roughly 70% of instances of secondary aplastic anemia happen as a result of idiosyncratic reactions to medication or chemical compounds. In idiosyncratic reactions the bone marrow failure is unpredictable and unrelated to dose. Some medication related to idiosyncratic secondary aplastic anemia are listed in Box 19. Further research is required to assess how these genetic variations, and other but undiscovered components, contribute to aplastic anemia. Pathophysiology the primary lesion in acquired aplastic anemia is a quantitative and qualitative deficiency of hematopoietic stem cells. Stem cells of sufferers with acquired aplastic anemia have diminished colony formation in methylcellulose cultures. The severe depletion of hematopoietic stem and progenitor cells from the bone marrow could additionally be due to direct harm to stem cells, immune injury to stem cells, or other unknown mechanisms. Young and colleagues confirmed that environmental exposures could alter selfproteins, induce expression of abnormal or novel antigens, or induce an immune response that cross-reacts with selfantigens. Candidate antigens have been recognized from aplastic anemia affected person sera, including kinectin,35 diazepam-binding inhibitor-related protein 1,36 and moesin. Approximately one-third of patients with acquired aplastic anemia have shortened telomeres in their peripheral blood granulocytes compared with age-matched controls. Patients usually current with symptoms of insidious-onset anemia, with pallor, fatigue, and weak point. Severe and prolonged anemia can lead to critical cardiovascular problems, together with tachycardia, hypotension, cardiac failure, and death. Symptoms of thrombocytopenia are additionally varied and embody petechiae, bruising, epistaxis, mucosal bleeding, menorrhagia, retinal hemorrhages, intestinal bleeding, and intracranial hemorrhage. Fever and bacterial or fungal infections are unusual at preliminary presentation however could happen after extended intervals of neutropenia. Laboratory Findings Pancytopenia is typical, though initially only one or two cell lines could additionally be decreased. The serum iron level and p.c transferrin saturation may be increased, which reflects decreased iron use for erythropoiesis. Liver operate take a look at outcomes may be abnormal in instances of hepatitis-associated aplastic anemia. In patients receiving immunosuppressive therapy, the chance of growing an abnormal karyotype is 14% at 5 years and 20% at 10 years. Treatment and Prognosis Severe acquired aplastic anemia requires quick attention to forestall critical problems. Further studies are presently underway to consider the efficacy of eltrombopag in pediatric extreme aplastic anemia. Other supportive remedy consists of antibiotic and antifungal prophylaxis in circumstances of prolonged neutropenia. Patients with mild to moderate aplastic anemia may not require therapy but have to be monitored periodically for pancytopenia and irregular cells. The overall end result for sufferers with acquired aplastic anemia has dramatically improved prior to now 20 years. The three commonest inherited/congenital bone marrow failure issues related to pancytopenia are Fanconi anemia, dyskeratosis congenita, and Shwachman-Bodian-Diamond syndrome. Guido Fanconi first described this syndrome in three brothers with pores and skin pigmentation, short stature, and hypogonadism. The symptoms related to pancytopenia usually become obvious at 5 to 10 years of age, though some sufferers might not present till maturity. This contains an increased incidence of leukemia in childhood and solid tumors. Laboratory results are just like those in acquired aplastic anemia, with pancytopenia, reticulocytopenia, and a hypocellular bone marrow. However, the precise role of telomere shortening in the evolution of bone marrow failure and most cancers is at present unclear. Patients must also have decreased intensity pretransplant conditioning due to their underlying chromosomal instability.
The valve is prepped on the back desk as per producer specifications and reverse-mounted (as in contrast with aortic valve delivery) on the Commander delivery catheter treatment toenail fungus discount rocaltrol 0.25 mcg without a prescription. The most technically challenging part of this procedure is positioning of the Sapien valve treatment quadriceps tendonitis best 0.25 mcg rocaltrol. As the valve expands treatment 2015 0.25 mcg rocaltrol purchase amex, it shortens from the inflow facet while the outflow aspect stays unchanged in place. The middle balloon marker on the Sapien valve and central wire on the degenerated BioP valve will serve as radiographic markers and positioning must be achieved in the method described earlier, however taking these two radio-opaque landmarks into consideration. Medical therapy after ViV consists of systemic anticoagulation with warfarin over the long term, though others have reported using dual antiplatelet therapy alone. Most of these sufferers have had prior sternotomies or have comorbidities that preclude surgical intervention. In the longer term, we expect to see improved design and application of the remedy and larger-scale scientific trials to reply the questions of efficacy and durability in appropriately selected sufferers. Contemporary trends in the use and outcomes of surgical therapy of tricuspid regurgitation. Six-month end result after transcatheter edge-to-edge repair of extreme tricuspid regurgitation in sufferers with coronary heart failure. Venous entry, creation of a rail, advancement, and mounting of the valve are much like the steps for the previously described ViV procedure. Transcatheter tricuspid valve restore with a new transcatheter coaptation system for the therapy of extreme tricuspid regurgitation: 1-year clinical and echocardiographic outcomes. Percutaneous tricuspid valve regurgitation restore with the MitraClip gadget utilizing an edge-to-edge bicuspidization approach. Transcatheter tricuspid valve restore with the MitraClip system using intracardiac echocardiography: proof of idea. Mitral loop cerclage annuloplasty for secondary mitral regurgitation: first human outcomes. Trends and outcomes of tricuspid valve surgical procedure in North America: an analysis of more than 50,000 patients from the Society of Thoracic Surgeons database. Transcatheter tricuspid valve-in-valve implantation for the therapy of dysfunctional surgical bioprosthetic valves: an International, Multicenter Registry research. Transcatheter valve-inring implantation for the therapy of residual or recurrent tricuspid valve dysfunction after prior surgical repair. Transcatheter tricuspid valve restore: new valve, new opportunities, new challenges. Association of tricuspid regurgitation with transcatheter aortic valve alternative outcomes: a report from the Society of Thoracic Surgeons/American College of Cardiology transcatheter valve remedy registry. Three-dimensional geometry of the tricuspid annulus in wholesome subjects and in patients with useful tricuspid regurgitation: a real-time, three-dimensional echocardiographic examine. Recommendations for noninvasive analysis of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. The worldwide multicenter trivalve registry: which patients are present process transcatheter tricuspid restore Postprocedural adjustments of tricuspid regurgitation after MitraClip remedy for mitral regurgitation. Kapadia fifty eight � Hypertrophic cardiomyopathy is a disease course of that varies broadly in its clinical presentation and has been associated with many alternative genetic mutations. Patients at excessive threat for sudden cardiac demise must be considered for an implantable cardioverter-defibrillator. Careful consideration to anatomic particulars and appropriate selection of sufferers are requisites for procedural success. With improved understanding of the clinical heterogeneity of this course of, hypertrophic cardiomyopathy appears to be a more acceptable descriptive time period. Although there have been dramatic advances in understanding of the genetic predisposition for this illness state, the utility of genetic study for absolutely the diagnosis remains preliminary. However, the future holds promise that genetics will turn out to be a extra dependable software for establishing and confirming this prognosis. Given the heterogeneity of the illness course of even within the identical family, its medical course and long-term outcomes differ significantly. Therefore management strategies span the vary from close outpatient follow-up to surgical reworking of the myocardium. This presents a challenging dilemma when it comes to grasping the scientific course of this disorder. Often, the presentation lacks the basic options on echocardiography, and coexisting diagnoses that can trigger myocardial hypertrophy, similar to arterial hypertension and aortic stenosis, can also be present. However, the spectrum of disease additionally features a subset of sufferers with severe, life-limiting symptoms together with heart failure, arrhythmias, syncope, chest pain, and sudden demise. Selection bias performed a major role within the initial attempts to characterize patient outcomes. Earlier studies from tertiary referral centers implied ominously high annual mortality charges of 3% to 6%; nevertheless, this work was limited by a big referral bias. More generally, sufferers develop symptoms similar to angina, syncope, or exertional dyspnea. The etiology of microvascular dysfunction is probably multifactorial and due partly to arteriolar medial hypertrophy, which finally ends up in lowered luminal diameter, impaired coronary vasodilatory response, and a supply-demand mismatch because of an abnormally thickened ventricle. Hemodynamic mechanisms of syncope all result in a sudden and severe discount in cardiac output which will contain ischemia, outflow tract obstruction, or severe diastolic dysfunction. It is important to recognize this subset of sufferers, given the potential alteration in therapeutic technique. This is most likely brought on by the lack of atrial contraction, discount in diastolic filling time, and exacerbation of underlying ischemia. Elderly sufferers are sometimes discovered to have an elliptical ventricular cavity with hypertrophy predominantly of the basal septum. In distinction, younger sufferers (<55 years) often have a crescent-shaped ventricular cavity associated with diffuse hypertrophy of the interventricular septum. Obstruction will not be current underneath resting situations however can be provoked by pharmacologic. It is most useful to sweep anterior to posterior with continuous Doppler imaging to distinguish these two flows. This is manifested by decreased maximal circulate velocity in early diastole, an increase in isovolumic relaxation time, and an increased atrial contribution to ventricular filling. Furthermore, scarring is proscribed to the areas of abnormal hypertrophy, and the diploma of scarring is proportional to the magnitude of hypertrophy, whereas wall thickening was inversely associated. Catheterization is often used, nonetheless, if noninvasive imaging is of inadequate quality to quantify the diploma or location of obstruction, to evaluate for coronary illness earlier than a deliberate surgical therapy. Use of a wire by way of a information catheter usually results in increased management in the course of the pullback and a more correct determination of the level of obstruction. Given the fact that numerous studies have recognized particular genetic mutations (Table 58. However, significant limitations, together with selection bias, the small variety of included familial cohorts, low frequency of particular gene mutations, and variability of the phenotypic product, have hindered most genotype-phenotype correlation studies. If a known pathogenic mutation is discovered within the affected person, family members could also be screened for a similar mutation, thus elucidating their risk of growing scientific manifestations. This in turn can information planning of follow-up examinations and discussions relating to participation in aggressive sports activities for family members of affected sufferers. Second, sufferers with atypical scientific features can endure genetic testing to consider for a nonsarcomeric genetic mutation (causing so-called "phenocopy" conditions). An enhance in left ventricular systolic pressure is accompanied by a lower within the arterial pulse stress, due to exacerbation of the dynamic outflow gradient after increased diastolic filling time after a untimely ventricular contraction in a affected person with hypertrophic cardiomyopathy. The red tracing represents left ventricular strain, and the blue tracing represents aortic stress. Their adverse chronotropic effect leads to increased diastolic filling time, which reduces left atrial pressure and may enhance congestive symptoms related to diastolic dysfunction. The negative inotropic impact of these brokers results in reduced myocardial oxygen consumption with a resultant lower in anginal signs.
Cacliadoce (Carqueja). Rocaltrol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97071
The nuclei of those cells are usually large treatment kidney infection rocaltrol 0.25 mcg discount without a prescription, often with irregular distribution of chromatin medicine in motion quality rocaltrol 0.25 mcg, and so they might have an vague or jagged border treatment with cold medical term purchase rocaltrol 0.25 mcg otc, or there may be "blebbing" on the border. Increased mitosis may be shown by the presence of several mitotic figures in the cell button. Transudates Versus Exudates As noted, the accumulation of a great amount of fluid in a cavity known as an effusion. There are varied pathologic reasons for the formation of effusion and are because of both an increase in the production of the fluid or a decreased price of fluid absorption. In general, transudates develop as a half of systemic illness processes that affect the absorption or formation of the fluid in order that it accumulates, corresponding to congestive coronary heart failure15,16; whereas exudates point out inflammatory problems that intervene with reabsorption on the location the place the fluid originates, leading to fluid accumulation associated with bacterial or viral infections, malignancy, pulmonary embolism, or systemic lupus erythematosus. Proper willpower considerably aids in identifying the analysis, and literature does point out that other markers are being investigated to decide their diagnostic usefulness in differentiating the effusion. When an effusion is in the peritoneal cavity, it also may be referred to as ascites or ascitic fluid. Gross Examination Transudates should seem straw colored and clear, whereas the colour of exudates varies (yellow, green, pink/red) and it can seem cloudy. A cloudy effusion may indicate an infectious course of (leukocytes); bloody might indicate hemothorax, trauma, or malignancy; and milky often indicates the presence of chyle (fluid consisting of emulsified fats and lymph) within the pleural cavity. When neutrophils are seen, they could have extra segments and longer filaments than in peripheral blood. Mesothelial cells are the liner cells of body cavities and are shed into these cavities continuously. These are large (12- to 30-mm) cells and have a "fried egg" appearance with basophilic cytoplasm, oval nucleus with easy nuclear borders, stippled nuclear chromatin pattern, and one to three nucleoli. The nucleus-to-cytoplasm ratio is 1:2 to 1:three, and this is typically consistent regardless of the variability in cell size. These could additionally be present in giant numbers, nonetheless, because of allergic response or sensitivity to foreign materials. If possible, Gram staining should be carried out on a second cytocentrifuge slide to aid in fast identification if micro organism are discovered. Lupus erythematosus cells could additionally be seen in serous fluids of patients with systemic lupus erythematosus, as a result of all of the components essential for the formation of these cells-presence of the lupus erythematosus factor, incubation, and trauma to the cells-exist in vivo. A lupus erythematosus cell is an intact neutrophil that has engulfed a homogeneous mass of degenerated nuclear material, which displaces the traditional nucleus. Lupus erythematosus cells could additionally be present in synovial fluid simply as in serous fluid. As always, a careful search must be made for bacteria when many neutrophils are seen. If a crystal analysis is to be carried out, an aliquot of fluid should be removed for this objective before the hyaluronidase is added. Differential Cell Counts Cells present in regular synovial fluid are lymphocytes, monocytes/ histiocytes, and synovial cells. Synovial cells line the synovial Intracellular and extracellular crystals could also be current in synovial fluid and are clinically important. Crystal examination could also be performed by inserting a drop of fluid on a slide and adding a coverslip or by examining a cytocentrifuge preparation. All synovial fluids ought to be examined rigorously for crystals utilizing a polarizing microscope with a pink compensator. The crystals most commonly seen in synovial fluids are ldl cholesterol, calcium pyrophosphate, and monosodium urate. Cholesterol crystals are giant, flat, extracellular crystals with a notched nook. The procedure consists of introducing warmed saline into the lungs in 50-mL aliquots after which withdrawing it. The function of the procedure is to determine types of organisms and cells which are present in areas of the lung that are otherwise inaccessible. The specimen should at all times bear an intensive microbiologic workup and infrequently cytologic examination. It is common to see micro organism, yeast, or both on cytocentrifuge slides ready from these specimens. Because samples are obtained from the interior of the lung and will comprise airborne organisms, care ought to be taken to avoid aerosol manufacturing. Samples ought to be blended and containers opened underneath a biologic security hood, and a masks should be worn when performing cell counts. Significant cell deterioration happens inside 30 minutes of collection, with the neutrophils disintegrating most rapidly. Pneumocytes, which can resemble mesothelial cells or adenocarcinoma, could also be seen in patients with acute respiratory misery syndrome. Ciliated epithelial cells can be seen and must be reported as a result of they point out that the pattern was obtained from the upper respiratory tract as an alternative of deeper within the lung. These are columnar cells, with the nucleus at one end of the cell, elongated cytoplasm, and cilia at the opposite end of the cell from the nucleus. Histiocytes laden with carbonaceous material are seen in patients who use tobacco. Pneumocystis jirovecii (formerly Pneumocystis carinii) may be seen in specimens from sufferers infected with human immunodeficiency virus. Because of the viscosity of synovial fluid, it must be pretreated with hyaluronidate earlier than testing to liquefy the specimen for each automated and handbook test strategies. A whole of six nucleated cells are counted on both sides of the hemacytometer, with all 9 squares counted on both sides. The differential was 52% lymphocytes, 20% neutrophils, 22% monocytes, 4% myelocytes, and 2% blasts. On the cytocentrifuge preparation, there were several neutrophils and a few monocytes/ histiocytes. On the cytocentrifuge slide prepared from a peritoneal fluid sample, many giant cells are seen, singly and in clumps. The cells have a "fried egg" look and basophilic cytoplasm, and some are multinucleated. The crystals were needle formed and, when polarized with the use of the purple compensator, appeared yellow on the y-axis. Cell counting of body fluids: comparison between three automated haematology analysers and the manual microscope method. Discuss the significance of the history and bodily examination in diagnosis of anemia. Explain how the body adapts to anemia and the symptoms experienced by the patient. Distinguish amongst efficient, ineffective, and insufficient erythropoiesis when given examples. Explain the importance of analyzing the peripheral blood movie when investigating the cause for an anemia and distinguish important findings. Describe variations in purple blood cell morphology similar to inclusions and modifications in form, quantity, or color. Use an algorithm incorporating the absolute reticulocyte rely to specify three groups of anemias involving decreased or ineffective pink blood cell manufacturing and provides one instance of every. Use an algorithm incorporating the mean cell quantity to slim the differential prognosis of anemia. The physician asked the patient to schedule an appointment so that she may decide the purpose for the signs before offering therapy. Why did the doctor need the patient to come to the office before she prescribed remedy How do the imply cell volume and reticulocyte depend assist decide the classification of the anemia Why is the examination of the peripheral blood film important in the investigation of an anemia This article offers an overview of the mechanisms, analysis, and classification of anemia. Thus these swimming pools of "wholesome" individuals might lack the heterogeneity required to be universally applied to any considered one of these populations of individuals. Examples of hematologic reference intervals for the grownup and pediatric populations are included on the inside cover. They are listed based on age and intercourse, but race, environmental, and laboratory factors also can affect the values.
Syndromes
Midterm outcomes of endovascular repair of descending thoracic aortic aneurysms with firstgeneration stent grafts medicine lookup buy 0.25 mcg rocaltrol fast delivery. Treatment of type B aortic dissection: endoluminal repair or conventional medical therapy Complicated acute kind B aortic dissection: midterm results of emergency endovascular stent grafting medications gerd order rocaltrol 0.25 mcg. Endovascular repair of acute kind B aortic dissection: early and mid-term results medications emts can administer rocaltrol 0.25 mcg buy fast delivery. Endovascular restore of difficult acute type-B aortic dissection with stentgraft: early and mid-term outcomes. Midterm results after endovascular remedy of acute, complicated sort B aortic dissection: the Talent Thoracic Registry. Endovascular stent graft remedy of aortic dissection: determinants of postinterventional end result. Aneurysm of the descending thoracic aorta: replacement with using a shunt or bypass. Degenerative and atherosclerotic aneurysms of the thoracic aorta: determinants of early and late surgical consequence. Variables predictive of outcome in 832 patients undergoing repairs of the descending thoracic aorta. Risk of replacement of descending aorta with a standardized left heart bypass method. Surgical experience in descending thoracic aneurysmectomy with and with out adjuncts to avoid ischemia. Endovascular restore of thoracic aortic aneurysms: stent graft fixation throughout the aortic arch vessels. Initial experience with intentional stent graft protection of the subclavian artery throughout endovascular thoracic aortic repairs. Left subclavian artery management in endovascular restore of thoracic aortic aneurysms and aortic dissections. Transluminal placement of endovascular stent grafts for the treatment of descending thoracic aortic aneurysms. The "first generation" of endovascular stent grafts for patients with aneurysms of the descending thoracic aorta. Improved results of atherosclerotic arch aneurysm operation with a refined approach. Thoracic aortic aneurysms: treatment with endovascular self-expandable stent grafts. Transluminal stent graft placements for the treatment of acute onset and continual aortic dissections. Current administration and end result of persistent sort B aortic dissection: outcomes with open and endovascular restore for the explanation that introduction of thoracic endografting. Rapid pacing for higher placing: comparability of strategies for exact deployment of endografts within the thoracic aorta. Comparison of angiography, transesophageal echocardiography, and intravascular ultrasound. Intentional occlusion of the left subclavian artery throughout endovascular stent graft implantation in the thoracic aorta: risk and relevance. Retrograde sort A aortic dissection after endovascular stent graft placement of kind B dissection. Prognosis for patients with sort B acute aortic dissection: danger analysis of early requirement for elective surgery. Endovascular stent grafts for acute and chronic kind B aortic dissection: comparability of scientific outcomes. Acute and contained rupture of the descending thoracic aorta: remedy with endovascular stent grafts. Natural history, pathogenesis, and etiology of thoracic aortic aneurysms and dissections. Yearly rupture or dissection rate for thoracic aortic aneurysms: simple prediction primarily based on measurement. Thoracic aortic aneurysm and dissection: rising prevalence and improved outcomes reported in a nationwide population-based study of greater than 14,000 cases from 1987 to 2002. Surgical therapy of aneurysms of the descending thoracic aorta: long-term leads to 500 sufferers. Endovascular restore of descending thoracic aortic aneurysms: an early experience with intermediate-term follow-up. Endovascular grafts within the treatment of thoracic aortic aneurysms and pseudoaneurysms. Elective endovascular stent graft restore of atherosclerotic thoracic aortic aneurysms: scientific results and midterm follow-up. Endovascular stent graft repair of stomach and thoracic aortic aneurysms: a ten-year expertise with 817 sufferers. Endovascular exclusion of thoracic aortic aneurysms: mid-term results of elective remedy and in contained rupture. Stent graft placement in atherosclerotic descending thoracic aortic aneurysms: midterm outcomes. Midterm outcomes of endovascular therapy of sophisticated acute kind B aortic dissection. Endovascular remedy of kind B aortic dissection: the problem of late success. Midterm outcomes for endovascular restore of sophisticated acute and persistent kind B aortic dissection. Pathophysiology of paraplegia following endovascular thoracic aortic aneurysm repair. Changes in aneurysm morphology and stent graft configuration after endovascular repair of aneurysms of the descending thoracic aorta. Embolization of perigraft leaks after endovascular stent graft therapy of aortic aneurysms. Intentional left subclavian artery occlusion by thoracic aortic stent grafts without surgical transposition. Fenestration in endovascular grafts for aortic aneurysm repair: new horizons for preserving blood flow in department vessels. Aortic arch reconstruction by transluminally placed endovascular branched stent graft. Endovascular stent grafting after arch aneurysm repair using the "elephant trunk". Penetrating atherosclerotic ulcer of the aorta: remedy by endovascular stent graft placement. Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery: guidelines for the therapy of belly aortic aneurysms: report of a subcommittee of the Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. A multicenter controlled medical trial of open versus endovascular therapy of stomach aortic aneurysm. Mortality results for randomised controlled trial of early elective surgical procedure or ultrasonographic surveillance for small belly aortic aneurysms. Abdominal aortic aneurysm rupture rates: a 7-year follow-up of the whole belly aortic aneurysm population detected by screening. Endovascular restore of aortic aneurysm in patients bodily ineligible for open restore. A statewide experience with endovascular belly aortic aneurysm restore: speedy diffusion with wonderful early results. Outcomes of thoracic endovascular aortic repair in acute kind B aortic dissection: results from the Valiant United States investigational gadget exemption study. Treatment of chronic aortic dissection by transluminal endovascular stent-graft placement: preliminary results. Endovascular restore of complicated continual distal aortic dissection: intermediate outcomes and complications. Endovascular repair by custom-made branched stent-graft: a promising remedy for continual aortic dissection involving the arch branches. Outcomes after stent graft therapy for dissection-related aneurysmal degeneration in the descending thoracic aorta. Initial and midterm results of the Bolton relay thoracic aortic endovascular pivotal trial. The affect of female gender on the end result of endovascular abdominal aortic aneurysm repair.
Functional tricuspid regurgitation is common medicine misuse definition trusted rocaltrol 0.25 mcg, and customarily associated to pulmonary hypertension and/or left sided coronary heart valve disease medicine vicodin 0.25 mcg rocaltrol discount with mastercard. Surgery for isolated tricuspid valve illness has not been routinely undertaken-in part due to uncertainty regarding populations that benefit medications vaginal dryness discount 0.25 mcg rocaltrol free shipping, and the diploma of comorbidities that generally accompany important tricuspid valve disease. However, the appearance of percutaneous valve therapies have raised the chance of "beating-heart" procedures, perhaps without basic anesthesia, that will enable us to establish the sufferers acceptable for therapy, and the timing within which to undertake it. This examine was terminated before completion, due to an apparent extra of stroke and myocardial infarction in the therapy group. The inside anchor is deployed in the proper ventricular aspect of the myocardial septum, and the exterior anchor over the left ventricular free wall. The procedure is carried out in hybrid style by way of the interior jugular vein (for internal anchor) along with a mini-thoracotomy (for exterior anchor), with out the need for cardiopulmonary bypass. Pharmacologic therapies also may not totally handle the dynamic increase in left atrial pressure throughout heart failure exacerbations or throughout exercise. Two anchors, one deployed on the proper ventricular facet of the septum, and the other over the left ventricular free wall. They are secured by an inner anchor permitting ventricular plication without the necessity for cardiopulmonary bypass. Evidence in help of this notion comes from sufferers with mitral valve stenosis and coexisting atrial septal defect. They have fewer signs than mitral valve stenosis patients with an intact septum. Implantation was associated with a pulmonary artery to systemic (ascending aorta) blood flow ratio (Qp/ Qs) of 1. A larger trial that included heart failure sufferers with preserved (n = 8) and decreased ejection fraction (n = 30) was undertaken, and outcomes had been recently reported. There had been important enhancements in functional class at 3 and 12 months, without changes in left or right ventricular operate. There was, nonetheless, a discount or absence of left to proper atrial move recognized in 50% of individuals, associated to neointimal thickening and consequent fusion of the valve commissures. Importantly, useful improvement, morbidity, and mortality improvements had been noticed in these with patent shunts. A second-generation gadget has been created and not utilizing a central valve, and histological research have revealed no vital pannus infiltration at 6 months. Other interatrial shunt units have been created, and are being investigated for heart failure and pulmonary hypertension. It is implanted into a branch of the pulmonary artery using a specialized delivery system throughout a right heart catheterization. It has no battery and is powered by a radiofrequency sign from outside of the physique. Pressure information are transmitted wirelessly to a safe web site, where physicians and nurses can view discrete knowledge or pressure tendencies graphed longitudinally over time. During the primary 6 months after randomization, there was a 28% discount within the danger of heart failure hospitalizations for the remedy group compared with the management group (P <. During the entire single-blinded follow-up interval, averaging greater than 15 months, the remedy group demonstrated a big 37% decrease in the price of heart failure hospitalizations in contrast with the management group. Postapproval observational knowledge suggest that the efficacy of this type of ambulatory monitoring continues to be related to reductions in heart failure admissions and overall heart failure prices. The sensor lead is implanted utilizing a transvenous approach and transseptal crossing of the interatrial septum, putting the tip of the sensor system lead in the left atrium. Patients had been randomized to system implantation and pressure-guided therapy, or optimum medical remedy with a reminder module. There were concerns concerning the frequency of procedural related problems which prompted early trial termination. However, the device-guided remedy group did exhibit a pattern toward decreased general heart failure hospitalizations. Percutaneous therapy for tricuspid regurgitation: a brand new frontier for interventional cardiology. Many of these devices remain underneath investigation, but even if only a few succeed, the means forward for this new field of interventional heart failure will be bright. Heart disease and stroke statistics-2014 replace: a report from the American Heart Association. Forecasting the influence of heart failure in the United States: a coverage statement from the American Heart Association. Chronic baroreflex activation: a potential therapeutic method to coronary heart failure with preserved ejection fraction. Chronic baroreflex activation results on sympathetic nerve visitors, baroreflex perform, and cardiac haemodynamics in coronary heart failure: a proof-of-concept research. Transvenous phrenic nerve stimulation for the treatment of central sleep apnoea in heart failure. Mechanisms and clinical consequences of untreated central sleep apnea in heart failure. Survival after aortic valve replacement for severe aortic stenosis with low transvalvular gradients and severe left ventricular dysfunction. Transcatheter aortic valve alternative: current views and future implications. Transcatheter aortic valve substitute versus surgical valve alternative in intermediate-risk sufferers: a propensity rating evaluation. Secondary mitral and tricuspid regurgitation accompanying left ventricular systolic dysfunction: is it necessary, and how is it treated Effects of carvedilol on left ventricular mass, chamber geometry, and mitral regurgitation in persistent coronary heart failure. Effect of cardiac resynchronization remedy on left ventricular dimension and function in chronic coronary heart failure. Percutaneous repair of the tricuspid valve using a novel cinching system: acute and chronic expertise in a preclinical giant animal mannequin. Transcatheter remedy of severe tricuspid regurgitation using the edge-to-edge restore technique within the presence and absence of pacemaker leads. Surgical ventricular restoration in the treatment of congestive coronary heart failure as a outcome of post-infarction ventricular dilation. Percutaneous left ventricular partitioning in patients with persistent coronary heart failure and a prior anterior myocardial infarction: outcomes of the percutaneous ventricular restoration in continual heart failure patients trial. New less invasive ventricular reconstruction approach in the treatment of ischemic heart failure. Interatrial Shunting for Treating Heart Failure: Early and Late Results of the First-in-Human Experience With the V-Wave Interatrial Shunt System. Transcatheter therapy of coronary heart failure with preserved or mildly decreased ejection fraction utilizing a novel interatrial implant to decrease left atrial strain. Clinical consequence of transcatheter therapy of coronary heart failure with preserved or mildly reduced ejection fraction utilizing a novel implant. Wireless pulmonary artery strain monitoring guides administration to cut back decompensation in coronary heart failure with preserved ejection fraction. Ambulatory hemodynamic monitoring reduces coronary heart failure hospitalizations in "Real-World" clinical apply. Direct left atrial pressure monitoring in ambulatory heart failure patients: initial expertise with a new everlasting implantable gadget. Direct left atrial stress monitoring in severe heart failure: long-term sensor performance. Physician-directed patient self-management of left atrial stress in superior continual coronary heart failure. Wireless pulmonary artery haemodynamic monitoring in chronic coronary heart failure: a randomised managed trial. Hemodynamic basis of train limitation in patients with coronary heart failure and normal ejection fraction. Masked left ventricular restriction in elderly sufferers with atrial septal defects: a contraindication for closure
The efflux of those ions results in symptoms ketosis purchase rocaltrol 0.25 mcg on-line water efflux and intracellular dehydration medications peripheral neuropathy cheap rocaltrol 0.25 mcg amex, successfully rising the intracellular concentration of Hb S and intensifying polymerization medications elavil side effects generic rocaltrol 0.25 mcg visa. Another contributor to K1 and Cl2 efflux and the resultant dehydration is the K1/Cl2 cotransporter system (Kcc1). Ironically, this system is activated by dehydration and positively charged hemoglobins similar to Hb S and Hb C. The K1/Cl2 cotransporter pathway can also be activated by the low pH encountered in the spleen and kidneys. One potential clarification for the altered operate of the membrane channels is oxidative harm triggered by Hb S polymerization. This uneven distribution of membrane phospholipids is completed by adenosine triphosphatedependent enzymes known as translocases or flippases (Chapter 6). Inhibition of flippases and activation of an enzyme known as scramblase cause a extra random distribution of membrane phospholipids, which increases the number of choline phospholipids on the inside half of the membrane and the number of aminophospholipids on the exterior membrane surface. Microparticles are generated when these cells endure stimulation, activation, or apoptosis. They type a posh biosystem that participates in cellular communication in normal and pathologic conditions after their phagocytosis by other cells, their binding to cell floor receptors, or their fusion with the cell membrane of target cells. Inflammation and vasoocclusive crisis can induce the release of microparticles, which might, in turn, additional modulate the inflammatory response. It is feasible that the detection, quantification, and identification of microparticle subtypes could probably be used diagnostically or prognostically to predict medical outcomes. Chronic hemolysis (intra- and extravascular) trigger a rise in free heme iron and stimulates synthesis and release of erythropoietin. Symptoms additionally range between ethnic teams with Indian patients expressing a a lot milder disease than their African counterparts. These eight clinically significant forms are listed in the order of severity and can have excessive morbidity and mortality charges. Various crises might happen: vasoocclusive or "painful," splenic sequestration, continual hemolytic, megaloblastic, and aplastic. Painful episodes manifest most frequently in bones, lungs, liver, spleen, penis, eyes, central nervous system, and urinary tract. Vasoocclusion may be triggered by any of these elements underneath numerous circumstances. Another mechanism of obstruction may be dense cells, which are less deformable and are at best risk for intracellular polymerization because of their higher Hb S focus. Endothelial adherence correlates considerably with the severity of painful episodes. In addition, sickle cell adherence to vascular endothelium ends in intimal hyperplasia that may gradual blood circulate. Splenic sequestration is characterised by a sudden trapping of blood in the spleen, which finally ends up in a fast decline in hemoglobin, usually to lower than 6 g/dL. This phenomenon occurs most frequently in infants and young kids whose spleens are chronically enlarged. Children experiencing splenic sequestration episodes could have earlier onset of splenomegaly and a lower level of Hb F at 6 months of age. Repeated splenic infarcts produce scarring leading to diminished splenic tissue and abnormal function. Loss of splenic perform contributes to an increased risk of bacterial infections. Sickle cells and vasoocclusion additional lower pulmonary blood circulate and alveolar oxygen tension, inflicting additional polymerization, thus exacerbating the syndrome. Creatinine and liver function exams are used to monitor organ perform and predict organ failure primarily from fats emboli. Treatment and continuous monitoring should be promptly initiated to cut back morbidity and mortality. Oxygen is run to preserve saturation at 95% and intravenous fluids to stop dehydration. Pain aid is crucial but opioids can cut back respiration so overdosing is averted. Incentive spirometry and chest physiotherapy are helpful to maintain enough air flow. Respiratory infection is presumed so antibiotics are prescribed to all patients and tailor-made to deal with confirmed infections. Necrotic bone marrow material and fats particles are launched into circulation and deposit within the lung, the place they fragment. Small fats droplets reenter circulation through pulmonary capillaries and terminate in various organs, causing harm. It is thought that these fats emboli produce organ ischemia, stimulating the discharge of vasoactive amines and inflammatory mediators. In addition to bone marrow and lung injury, patients typically experience neurologic (brain) and renal injury. Chemical evaluation shows elevated lactate dehydrogenase, ferritin, creatinine, alkaline phosphatase, and bilirubin, indicating end organ harm. A bone marrow evaluation is diagnostic showing myeloid necrosis, focal hypoplasia, lack of fats, and eosinophilic materials within the background. Fiberoptic bronchoscopy and bronchial lavage present intracellular fats in macrophages, and magnetic resonance imaging demonstrates the characteristic "star area" sample indicating infarction. In distinction, delayed analysis and therapy often ends in dying or permanent neurologic damage. Acute infections are frequent causes of hospitalization and have been the most common causes of death, especially within the first three years of life. Continuous screening and removal of sickle cells by the spleen perpetuate the persistent hemolytic anemia and autosplenectomy impact. Because other situations (such as hepatitis and gallstones) might trigger jaundice, continual hemolysis is tough to diagnose in sickle cell patients. Megaloblastic episodes result from the sudden arrest of erythropoiesis caused by folate depletion. Aplastic episodes (bone marrow failure) are the commonest life-threatening hematologic complications and are often related to infection, significantly parvovirus infection. When the bone marrow is suppressed quickly by bacterial or viral infections, however, the hematocrit decreases substantially with no reticulocyte compensation. If anemia is extreme and the bone marrow stays aplastic, transfusions are essential. Patients additionally experience cardiac defects, together with enlarged coronary heart and heart murmurs. In sufferers with severe anemia, cardiomegaly can develop as the center works harder to preserve sufficient blood move and tissue oxygenation. Increased cardiac workload together with elevated bone marrow erythropoiesis increases calorie burning, contributing to a reduced development price. Ulcers tend to heal slowly, develop unstable scars, and recur on the similar website, becoming a continual downside, with related chronic ache. Neurologic examination adopted by magnetic resonance imaging and, if out there, transcranial Doppler ultrasonography or magnetic resonance angiography is recommended to detect microstrokes. When proliferative retinopathy is detected, laser photocoagulation is performed and vitrectomy can be accomplished to resolve extreme vitreous hemorrhage. This lowered oxygen tension causes the cells to sickle, which finally ends up in damage to the cells. One explanation for this phenomenon is that the infected cell is uniquely sickled and destroyed, most likely in an area of the spleen or liver, the place phagocytic cells are plentiful, and the oxygen pressure is considerably decreased. There is moderate to marked polychromasia with a reticulocyte rely between 10% and 25%, corresponding with the hemolytic state and the resultant bone marrow response. Serum ferritin ranges are normal in younger sufferers however are probably to be elevated later in life. Chronic hemolysis is evidenced by elevated levels of indirect and whole bilirubin with the accompanying jaundice. An older screening take a look at detects Hb S insolubility by inducing sickle cell formation on a glass slide. A drop of blood is blended with a drop of 2% sodium metabisulfite (a reducing agent) on a slide, and the combination is sealed beneath a coverslip. The most typical screening check for Hb S, known as the hemoglobin solubility test, capitalizes on the decreased solubility of deoxygenated Hb S in resolution, producing turbidity.






