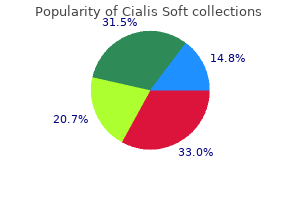
Cialis Soft
Cialis Soft
Cialis Soft dosages: 40 mg, 20 mg
Cialis Soft packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Both ends of the suture are then handed through the ipsilateral posterior vaginal apex and held with a hemostat impotence natural treatments proven 20 mg cialis soft. This repair is usually carried out along side a culdoplasty or uterosacral suspension erectile dysfunction 55 years old purchase cialis soft 20 mg on-line. The process could be simply tailored for a particular prolapse treatment erectile dysfunction faqs cheap 40 mg cialis soft amex, depending on the extent of the vault prolapse and whether or not coexistent anterior and posterior vaginal wall defects are current. The objective of any vault suspension ought to be to recreate a well-supported, functional vagina of acceptable size. The complexity of such a repair is predicated on how a lot coexistent anterior and posterior vaginal wall eversion is present. Such a scenario requires a much more complicated repair to reconstruct a useful, well-supported vagina of acceptable size. Over the years, intraperitoneal procedures used to help or droop the vaginal apex, as nicely as handle apical or posterior enteroceles, have developed. A McCall culdoplasty (see Chapter 53), initially described in 1957, stays a good procedure that can be used at the time of a vaginal hysterectomy as a outcome of it suspends the vagina to the plicated distal parts of the uterosacral ligaments. A traditional excessive uterosacral suspension makes an attempt to cross sutures bilaterally through the uterosacral ligament on the degree of the ischial spine. More just lately, the technique has been modified so that sutures are passed higher and more medially. This modified excessive uterosacral suspension has, in my view, led to the creation of a deeper vagina and significantly decreased the rate of ureteral compromise. Downward traction on the Allis clamp allows palpation of the uterosacral ligament on all sides. The ischial spines are palpated transperitoneally, and the ureter can usually be palpated alongside the pelvic sidewall wherever from 1 to 5 cm ventral and lateral to the ischial spine. Two to three delayed absorbable sutures are passed by way of the uppermost portion of the uterosacral ligament on each side. Traction on these sutures will allow movement of the affected person with no tension or pulling on the lateral pelvic aspect wall, theoretically reducing the potential for ureteral compromise. The delayed absorbable sutures that previously had been passed through the uterosacral ligament are individually brought out by way of the full thickness of the posterior vaginal wall. Such a state of affairs simply requires excision of the enterocele sac and closure of the defect at the stage of the neck. Fifty p.c of the length of the anterior and posterior vaginal partitions is everted. Such a situation would require suspension of the apex to the extent of the ischial backbone, in conjunction with restoration of support of the upper portion of the anterior and posterior vaginal partitions. Complete vaginal vault prolapse with full eversion of the anterior and posterior vaginal walls. Such a scenario requires a a lot more complicated repair, in that the prolapsed vaginal vault now must be suspended high up into the pelvic cavity to the level of the ischial spines. This must be accomplished along side other procedures that would need to be performed to provide durable assist to the anterior and posterior vaginal walls. Note that the suture is passed above and medial to the ischial spine, incorporating the coccygeus-sacrospinous ligament complex or the presacral fascia. Note that the suture is handed by way of the higher portion of the uterosacral ligament slightly below the extent of the ischial backbone. Note proper placement of suture into uppermost portion of uterosacral ligament (arrows). The vaginal wall is dissected off the underlying tissue, and the enterocele sac is identified and opened. A retractor is used to lift the sponges up out of the lower pelvis, thus fully exposing the cul-de-sac. When appropriate traction is positioned downward on the uterosacral ligaments with an Allis clamp, the uterosacral ligaments are easily palpated bilaterally. The anterior colporrhaphy is begun by initiating a dissection between Continued the prolapsed bladder and the anterior vaginal wall. The uterosacral suspension sutures are then tied elevating the prolapsed vaginal wall into the hole of the sacrum. The relationship between the intermediate portion of the uterosacral ligament and the ureter. The relationship between the ureter and the uppermost portion or the most proximal portion of the uterosacral ligament. Note the relationship of the uterosacral ligament to the proper ureter considered laparoscopically. The enterocele sac has been entered, and the cul-de-sac is being palpated in preparation for excising the peritoneal sac. The intraperitoneal contents have been packed with large laparotomy tail sponges to facilitate publicity of the posterior cul-de-sac. Note the excellent elevation of the apex of the vagina excessive up into the hollow of the sacrum, without any vital distortion of the vaginal axis. A massive retractor has been placed intraperitoneally, and the lap sponges have been elevated excessive up into the abdomen, thus nicely exposing the entire cul-de-sac. The proper uterosacral ligament has been identified, and a delayed absorbable suture has been handed by way of the best uterosacral ligament on the stage of the ischial backbone. The left uterosacral ligament has been recognized, and a delayed absorbable suture has been passed through the ligament at the level of the ischial spine. The distal portion of the cul-de-sac has been plicated across the midline with permanent sutures. Note that the cul-de-sac is being palpated and extra posterior vaginal pores and skin and peritoneum are being excised. The distal portion of the cul-de-sac is visualized in preparation for midline plication. A permanent suture is being handed across the cul-de-sac to plicate the distal parts of the uterosacral ligaments. The permanent sutures that have been beforehand passed to plicate the distal portions of the uterosacral ligaments are now tied within the midline, creating midline support of the cul-de-sac. The sutures that had been beforehand handed via the higher portion of the uterosacral ligament are actually individually taken out by way of the posterolateral features of the vaginal vault. Note the excellent elevation of the apex of the vagina into the hollow of the sacrum with none vital distortion of the vaginal apex. Note the conventional help of the anterior vaginal wall after the apical sutures have been tied. Patient with full uterine procidentia and vaginal eversion extending eleven cm past the introitus. View of the suspended C vaginal vault after vaginal hysterectomy with repairs and modified excessive uterosacral vaginal vault suspension. Vagina has been trimmed; note one pair of uterosacral suspension sutures has been brought by way of the anterior vaginal wall. Uterosacral suspension sutures have been tied; note excellent assist of anterior vaginal wall with dimpling where the uterosacral stitches have been brought out the anterior vaginal wall. Complete eversion of anterior vaginal wall; note uterosacral stitches have been tagged and shall be brought out by way of the anterior vaginal wall. Cross-section of the pelvis after excision of the enterocele sac and suspension of the vaginal apex to the uppermost portions of the uterosacral ligaments. The advantages of these procedures are that they can be performed quickly with minimal morbidity, usually with the affected person under a local anesthetic. A LeFort partial colpocleisis is an possibility if the affected person has her uterus and is not sexually energetic. Because the uterus is retained, evaluating any future uterine bleeding or cervical pathologic abnormalities is difficult. Therefore endovaginal ultrasound or endometrial biopsy, in addition to a Papanicolaou smear, should be carried out before surgery. A pudendal nerve block can be utilized if the procedure is being carried out with the affected person underneath native anesthetic. A Foley catheter with a 30-mL balloon is positioned for easy identification of the bladder neck. A mirror picture on the posterior facet of the cervix and vagina is also recognized. These flaps must be thin, leaving the utmost quantity of fascia on the bladder and rectum.
Viral assembly follows a sequence similar to erectile dysfunction treatment ayurveda cheap cialis soft 20 mg without prescription that of picornaviruses in a cellular membrane compartment erectile dysfunction treatment pdf generic 20 mg cialis soft free shipping. Transcription and replication are integrated into a single process utilizing a double rolling circle mechanism erectile dysfunction pills australia purchase cialis soft 20 mg on-line. The ranges of endemicity closely correlate with hygienic and sanitary circumstances of every geographic area. During primary an infection, the preliminary pathway of antiviral immune response is essentially unknown. Initial viral an infection is associated with activation of innate immunity within the liver. Since this antiviral response is likely related to a noncytopathic mechanism, little or no hepatocellular harm is obvious. Innate immunity additionally performs a crucial role within the activa tion of the adaptive immunity including humoral and cellular responses. Induction of a humoral immune response with pro duction of neutralizing antibodies prevents viral unfold and leads to subsequent elimination of circulating viruses. Class I molecules on the hepatocytes and cause scattered apop tosis of hepatocytes. The predominant infiltrating effector cells are macrophages, which most likely mediate the vast majority of hepatocellular harm. Following infection, the hepatotrophic viruses give rise to similar scientific, biochemical and pathological features. The clinical course ranges from an asymp tomatic illness to fulminant hepatitis and is typified by three phases, prodromal, symptomatic and convalescent, lasting from 6 weeks to 6 months. The major biochemical abnormality is an acute rise in serum alanine and aspartate aminotransferases, markers of hepatocellular necrosis, to higher than 2. Central and East Asia and North Africa/Middle East are estimated to have a high prevalence (>3. The basic pathological options of acute viral hepatitis are swollen hepatocytes, apoptotic hepatocytes (acido phil bodies), and the presence of inflammatory cells inside the hepatic lobule, predominantly lymphocytes and macrophages, which end in distortion of the traditional liver architecture. Treatment of acute viral hepatitis is supportive with the aim to keep sufficient vitamin, hydration and monitoring for the event of fulminant hepatitis. Treatment of acute hepatitis C must be thought of due to the excessive propensity to develop chronic hepatitis. Translation of the genome yields a single polyprotein, divided into three primary practical domains (P1, P2 and P3) from which nine or extra particular person viral proteins are cleaved. The hepatitis B virus open reading frames: preC and C (precore and core proteins), P (polymerase protein), preS1, preS2, and S (L, M, and S surface envelope proteins), and X protein are shown. The polymerase protein is covalently attached to the 5 of the strand and a capped oligoribonucleotide (spiral line) to the (+) strand. The outer traces represent the 4 transcripts, all terminating at a typical polyadenylation site. Reverse transcription happens, and the mature virions are assembled within the endoplasmic reticulum, the place they acquire the surface proteins. Cellular proteases in the endoplasmic reticulum catalyze the cleavage of the structural proteins, whereas viral encoded proteases cleave the nonstructural proteins. The extremely conserved core protein is the putative viral nucleocapsid and encompasses the first 191 amino acids of the polyprotein. The E1 and E2 are envelope glycoproteins with Cterminal hydrophobic transmembrane domains. The virion attaches and enters the hepatocyte and is internalized by way of clathrinmediated endocytosis. Initial attachment to the cell is by way of an interaction with the low density lipoprotein receptor and glycosaminoglycans present on heparan sulphate proteoglycans. The virions are then secreted by way of an unknown exocytotic pathway, most likely involving lipoprotein and not passing through the Golgi compartment. The genome is organized into three overlapping open reading frames flanked by 5 and 3 noncoding areas and a three polyadenylation. An antibody response may be demonstrated as early as week four however extra generally by week 12 coinciding with the onset of clinical symptoms. The presence or absence of each of those antigens and antibodies serologically defines the stage of sickness as acute, continual or recovered. It usually seems in serum 1�10 weeks after acute publicity and 2�6 weeks before the onset of symptoms. Following acute exposure to the virus, viral excretion is detectable within 2 weeks in serum and stool. The biopsy demonstrates typical options of acute viral hepatitis with a gentle inflammatory infiltrate, ballooning degeneration, scattered acidophil bodies and mild lobular disarray. Upper left insert shows a high power view of an acidophil physique with densely eosinophilic, irregularly shaped cytoplasm and pyknotic nucleus. There is type of complete involvement of the acini with extensive lack of parenchyma. Islands of hepatocytes are seen, separated by reticulin and inflammatory cells that kind bridges. Note ballooned hepatocytes along with scattered acidophil our bodies (towards the middle of biopsy). Unfortunately, most sufferers with persistent hepatitis B remain undiagnosed because of the dearth of inhabitants screening. Viral suppression can markedly enhance long-term outcomes and reduce the rate of demise, cirrhosis, liver transplant, and liver cancer. Currently, with the advent of noninvasive tests such as elastography, liver biopsy is performed or wanted in a definite minority of patients. The elastography, imaging, blood check, and/or biopsy data can be utilized to counsel sufferers about the probabilities of creating cirrhosis, cancer, the necessity for transplant, and the risk of illness transmission, in addition to the potential for identifying additional diagnoses. A 26-year-old man who had a history of greater than 50 sexual partners introduced with elevated liver enzymes that normalized after 1 month of follow-up. She rapidly developed coma throughout the ensuing 6 weeks and underwent a liver transplant. A liver biopsy was carried out 6 months earlier than her clinical presentation with quickly progressive liver illness in her transplanted liver. The clinical course in this affected person was modified by the addition of a nucleoside analogue, lamivudine. Her jaundice, ascites, and abnormal coagulation checks corrected to normal inside 3 months of initiating antiviral remedy. She remains nicely 8 years later and a liver biopsy reveals early cirrhosis but no evidence of development by bodily examination or by liver synthetic abnormalities. The patient had a identified hepatoma at the time of liver transplant, which was a single lesion, less than 5 cm in diameter, without evidence of vascular invasion by four-phase computed tomography. The finding of vascular invasion often portends a poor prognosis and signifies that the patient may have stage four illness and subsequent risk for disseminated most cancers. The mandate for occupational safety, vaccination of adolescents, and training of people concerned in high-risk actions are additionally essential public well being insurance policies to forestall new infections and alter the epidemiology of this disease. The mononuclear infiltrate is composed predominantly of lymphocytes, which frequently forms aggregates or even distinct lymphoid follicles with germinal centers, and occasional plasma cells and eosinophils. Interface hepatitis, formerly generally known as "piecemeal necrosis," is characterized by chronic inflammation extending past the limiting plate of the portal tract and is also seen in this micrograph. The estimated danger of progression to cirrhosis varies considerably depending on the population studied; some of the cofactors believed to accelerate fibrosis development are proven. Once superior fibrosis/cirrhosis develops, then the patient is at elevated threat of developing hepatocellular carcinoma and/or liver failure, which is manifested clinically by decompensated cirrhosis. Quantitative core antigen immunoassay 396 pA R T 2 Gastrointestinal illnesses Table forty six. Drugs could cause hepatotoxicity in either a dosedependent, or a dose-independent (idiosyncratic) style. Idiosyncratic drug reactions happen hardly ever (in 1:10 000�1: 100 000 persons utilizing the specific drug). However, the clinical role and value of pharmacogenetics are simply starting to emerge. Acetaminophen (paracetamol) exemplifies a drug which is hepatotoxic in a dose-dependent manner. Acetaminophen is extraordinarily protected when taken throughout the really helpful doses (4 g/ day), but doses of 8�10 g/day might cause severe liver necrosis.

Table 25-11 summarizes the vital thing advantages and downsides of each approach (Ette and Williams erectile dysfunction treatment germany cialis soft 20 mg discount mastercard, 2004; Tett et al over the counter erectile dysfunction pills uk cheap 20 mg cialis soft with amex, 1998) erectile dysfunction psychological cialis soft 40 mg discount on-line. Indeed, sufficient experimental design and the supply of valid information are essential considerations in model selection and testing. For example, the experimental design ought to determine whether a drug is being eradicated by saturable (dose-dependent) or easy linear kinetics. Metabolic rate could be measured at various drug concentrations using an in vitro system (see Chapter 12). Curve A represents a sluggish preliminary decline because of saturation and a quicker terminal decline as drug concentration decreases. Curve C represents a dominating distributive section masking the effect of Time Plasma drug focus profiles because of distribution and metabolic process. Finally, a combination of A and C might approximate a tough general linear decline (curve B). For example, concluding linear metabolism primarily based only on curve B can be incorrect. Contrary to widespread belief, complex models tend to masks opposing variables that should be isolated and examined through higher experimental designs. In this case, a constant infusion till steady-state experiment would yield info on saturation with out the affect of initial drug distribution. The use of pharmacokinetic models has been critically reviewed by Rescigno and Beck (1987) and by Riggs (1963). A mannequin is a secondary system designed to check the primary system (real and unknown). The assumptions in a mannequin must be practical and according to physical observations. On the opposite hand, a simulation may emulate the phenomenon with out resembling the true bodily process. A simulation with out identifiable assist of the bodily system does little to assist understanding of the essential mechanism. Drug A follows first-order pharmacokinetics, whereas drug B follows nonlinear pharmacokinetics and saturation occurs at greater drug concentrations. The latter is used to predict pharmacokinetic parameter values for humans based on animal data. Another mannequin class is the mechanistic one, by which fashions goal to embrace as much information as attainable concerning the system that surrounds the data being studied. Published knowledge within the physiology literature relating to measurement (mass) of organs and blood flow to every organ and physique mass are used. Compartmental fashions are additionally mechanistic fashions that use a system of differential equations to describe drug disposition. Model-dependent pharmacokinetic parameters can thus be determined with completely different approaches. Pharmacokinetic parameters may also be determined using noncompartmental analyses based on statistical moment principle. The variance of the residence time can additionally be decided using statistical second theory primarily based on likelihood density perform. After an intravenous bolus dose (500 mg) of an antibiotic, plasma�time concentration knowledge were collected and the area under the curve was computed to be 25 mg/L�h. What are the key considerations in fitting plasma drug data to a pharmacokinetic mannequin The most acceptable mannequin also depends on the objectives of the modeling train, in addition to the nature of the information that had been collected. For instance, a few of the algorithms that employ linearization might converge more shortly than those who carry out no linearization; subsequently, outcomes could probably be obtained more quickly. When ought to individual compartmental evaluation be used quite than inhabitants analysis For example, knowledge from a group of subjects could be pooled collectively such that a imply concentration�time profile is created from this group. Differential equations have the advantage of being very adaptable to computer simulation without lots of mathematical manipulations. Why do we assume that drug concentrations in venous and arterial blood are the identical in pharmacokinetics The arterial blood containing the diluted drug then perfuses all the body organs by way of the systemic circulation. In biking by way of the body, the blood leaving a tissue (venous) usually has a decrease drug focus than the perfusing blood (arterial). Drug concentration within the venous blood quickly equilibrates with the tissue and will turn out to be arterial blood within the next perfusion cycle (seconds later) via the body. In pharmacokinetics, the drug focus is assumed to decline smoothly and continuously. The difference in drug concentration between arterial and venous blood reflects drug uptake by the tissue, and this distinction might have essential penalties in drug therapy, such as tumor remedy. The principal concerns are measurement, drugprotein binding, and maximum life span potential of the species. The goals of the modeling should at all times be stored in thoughts, and the only model that best explains the info ought to at all times be retained. Bonati M, Latini R, Tognoni G, et al: Interspecies comparability of in vivo caffeine pharmacokinetics in man, monkey, rabbit, rat, and mouse. Boxenbaum H: Interspecies scaling, allometry, physiological time, and the bottom plan of pharmacokinetics. A physiological pharmacokinetic analysis of the cotinine disposition, and effects on clearance and distribution in the rat. Gibaldi M, Perrier D: Noncompartmental evaluation primarily based on statistical second principle. New Approaches in Toxicity Testing and Their Application in Human Risk Assessment. Mahmood I: Application of allometric ideas for the prediction of pharmacokinetics in human and veterinary drug growth. Mahmood I: Critique of potential allometric scaling: Does the emperor have clothes Nakashima E, Yokogawa K, Ichimura F, et al: A physiologically based mostly pharmacokinetic model for biperiden in animals and its extrapolation to people. New insights into the pharmacokinetics and metabolism of (R,S)-Ifosfamide in cancer sufferers using a population pharmacokinetic-metabolism model. Applied Pharmacokinetics & Pharmacodynamics: Principles of Therapeutic Drug Monitoring. Sawada Y, Hanano M, Sugiyama Y, Iga T: Prediction of the disposition of 9 weakly acidic and six weakly basic medicine in humans from pharmacokinetic parameters in rats. Watanabe T, Kusuhara H, Maeda K, Shitara Y, Sugiyama Y: Physiologically based pharmacokinetic modeling to predict transporter-mediated clearance and distribution of pravastatin in people. Veng-Pedersen P, Gillespie W: the imply residence time of medicine in the systemic circulation. This web page deliberately left blank Appendix A: Applications of Software Packages in Pharmacokinetics Philippe Colucci and Murray P. Computer pace and storage capacity have doubled approximately each 2 years over the last forty years (Keyes 2006). Therefore, mathematical computation time has dramatically shortened over the same time frame. The elevated pace of computers in addition to their storage capability has led to the development of numerous laptop software packages that now permit for the speedy answer of difficult pharmacokinetic equations and fast modeling of pharmacokinetic processes. At its core, a software program program is a set of directions written in a pc language. These software program applications simplify tedious calculations and permit extra time for the development of latest approaches to information evaluation and pharmacokinetic modeling. In addition, laptop software can also be used for the development of experimental research designs, statistical information therapy, knowledge manipulation, graphical representation of knowledge, pharmacokinetic mannequin simulation, and projection or prediction of drug motion. Consequently, these enhancements at the aspect of improvements in the analytical evaluation of systemic drug concentrations and the capturing of pharmacodynamic parameters have led to a a lot better understanding of the pharmacokinetics and pharmacodynamics of medicine during drug improvement. These are the noncompartmental, the individual compartmental, and the inhabitants compartmental approaches. This methodology grew to become well-liked in the early Eighties and is based on the theory of statistical moments, which is a mathematical concept explaining the distribution of information (Gibaldi et al, 2007; Riegelman et al, 1980; Yamaoka et al, 1978). The method utilizes easy analyses that require little or no pc power if any.
This is a large vessel that emanates from the lower left facet of the aorta just cephalad to the widespread iliac artery bifurcation of the aorta erectile dysfunction pills generic 40 mg cialis soft. Similarly erectile dysfunction drugs and high blood pressure trusted cialis soft 20 mg, the first branches from the inferior mesenteric artery are large vessels erectile dysfunction treatment lloyds pharmacy purchase 40 mg cialis soft. Both proper and left ureters descend into the pelvis and occupy a position medial and parallel to the hypogastric arteries. Again, the ureter is medial and roughly parallel to the fossa at the stage of the obturator artery and nerve. The medial facet of the ureter is sandwiched between the uterine artery (anteriorly) and the vaginal artery (posteriorly). The ureter enters the higher portion of the cardinal ligament, which consists of condensed fats and fibrous tissue, honeycombed with venous sinuses. Special care must be taken when a laparoscopic stapling device is utilized to secure the infundibulopelvic ligaments. At the caudal finish of the obturator fossa, the ureter sinks deeper into the pelvis and is crossed from lateral to medial obliquely by the uterine vessels. The uterine vessels continue medially to attain the lateral margin of the uterus at the cervicocorporal junction. The ureter B enters the upper portion of the cardinal ligament, which consists of condensed fats and fibrous tissue, honeycombed with venous sinuses. The ureter passes beneath the bladder pillar (vesicouterine ligament) to enter the bottom of the urinary bladder obliquely (trigone). After the operator enters the retroperitoneal house (see Chapter 37), essentially the most handy point at which the ureter can be recognized is where it crosses lateral to and medial above the frequent iliac artery. Any procedure performed on or across the uterosacral ligaments must keep in mind the place of the ureter relative to the operative web site. Dissection of the ureter by way of the cardinal ligament is difficult because the ligament is honeycombed with thin-walled vessels. The ureter can be unroofed by clamping above and excising that portion of the cardinal ligament. The pubovesicocervical fascia overlying the anterior surface of the uterine cervix is incised superficially and transversely with a pointy scalpel blade. After the operator enters the retroperitoneal area (see Chapter 37), probably the most handy level at which the ureter may be recognized is where it crosses lateral to medial above the common iliac artery. By cautious dissection with a protracted tonsil clamp and with using an untied hammock of umbilical tape to provide counteraction, the ureter can be clearly viewed to the purpose of uterine artery crossover. The hypogastric plexus is variable in configuration but may be quite loosely separated into superior, center, and inferior divisions. The middle hypogastric plexus sometimes divides into two major nerve trunks coursing inferiorly throughout the presacral area. The inferior hypogastric plexus continues to descend into the decrease pelvis and joins with the pelvic plexus, receiving rectal, vesical, and uterine afferents and carrying sympathetic efferents. The segment of nerve between the 2 ligatures is dissected from its loose attachments to the underlying sacral bone. This hemorrhage is difficult to control as a result of these vessels are tough to clamp or suture. I suggest pushing a sterile chrome steel thumb tack into the sacrum, thereby compressing the vessels. The elevated ligature encircles the middle hypogastric plexus as it descends into the pelvis over the presacral area. The buildings overlying the anterior floor of the sacrum and the L5 vertebra are visualized. The scissors lie underneath the dissected left ureter (far lateral); the scissors tip factors to the takeoff (origin) of the inferior mesenteric artery. The proper ovarian vessels and the best ureter (below the vessels) cross the right iliac artery and descend into the pelvis on the proper lateral margin of the presacral area. To the left and above are the left widespread iliac vein and the inferior mesenteric vessels. The subject is irrigated with regular saline and is carefully examined for any bleeding. Care is taken to avoid encroaching on the best ureter or inferior mesenteric artery throughout closure. Section of these ligaments close to their origin on the junction of the higher vagina and the cervix has been advocated for the reduction of dysmenorrhea. Nevertheless, uterosacral transection is an easier operation to carry out and often is finished with the laparoscopic approach. The buildings that must be recognized to keep away from injury are the right and left ureters and the uterine arteries. The latter are millimeters from the anterolateral aspect of the uterosacral ligaments. The uterosacral transection may be performed by laser ablation or by electrosurgical cutting. The incision starts 4 to 5 mm distal from the locus where the ligament attaches to the uterus. Alternatively, the ligament may be doubly clamped and incised, and every finish suture-ligated with everlasting sutures. Pain fibers from the body of the uterus and the cervix are transmitted through the ligament, and ache is referred to the decrease back via these fibers via the pelvic nerves and hypogastric plexus. Cutting present (blend one) at 30 to forty W is utilized on the lateral edge for brief bursts to diminish conduction unfold of thermal damage. Note that the ablation is initiated far sufficient posteriorly to keep away from entry into the uterine artery. The sigmoid colon (medial) must be protected against conduction (electric current) harm. A phase of tissue (inset) may be sent to the pathology laboratory to doc excision and to determine whether any pathology exists throughout the ligament. The greatest demonstration of the ligaments could be produced only by pulling the uterus upward (cranially) and sharply dissecting within the anterior direction, as illustrated here. The lymph nodes sometimes sampled embody the external iliac, internal iliac, frequent iliac, obturator, and periaortic nodes. Next, nodal tissue is excised from the hypogastric artery, where it joins the exterior iliac artery to kind the widespread iliac artery. This may be done extraperitoneally by locating the inferior epigastric artery and tracing it to the iliac vessels on the point the place the vessels cross under the inguinal ligament. The peritoneum has been opened at the bifurcation of the proper frequent iliac artery. The scissor tip barely elevates the exterior iliac artery; the clamp points to the external iliac vein. The external iliac artery is retracted with a vein retractor to allow the node-containing fats to be excised between the artery and the underlying exterior iliac vein. The obturator fossa is exposed by gently elevating the exterior iliac vein with a vein retractor. The fats is carefully teased out of the fossa with a hoop forceps, and the obturator nerve and artery are exposed. The external iliac artery is followed cranially to reach its junction with the hypogastric artery. The bifurcation of the aorta is situated, and nodes are sampled between the aorta and vena cava and between the aortic bifurcation and the left common iliac vein. Periaortic nodes are sampled at and above the origin of the inferior mesenteric artery. The ureter lies near the aorta on the left aspect and should be recognized if the dissection carries over to the left aspect of the aorta. Fat and nodes between these vessels typically are sampled on the upper limits of the dissection. Note that the left ovarian veins drain into the left renal vein and override the ureter. After the ligament is split and the incision made following division of the round ligament is related, the psoas muscle and the exterior iliac artery can be exposed easily.
The transurethral approach includes the endoscope being inserted into the urethra and through the bladder into the peritoneum erectile dysfunction types purchase cialis soft 40 mg without a prescription. The benefit of this method is that this conduit is sterile but the drawback is that devices to perform a surgical procedure should be of limited measurement erectile dysfunction 60784 20 mg cialis soft buy. Transgastric peritoneoscopy and liver biopsy was performed in survival porcine examine erectile dysfunction neurological causes generic cialis soft 40 mg without a prescription. This was the primary study to show that the peroral transgastric strategy to the peritoneal cavity would possibly function a substitute for laparoscopy or laparotomy. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Once the necrotic cavity is cleared, the gastrotomy is left to close by secondary intention. Direct endoscopic necrosectomy for the treatment of walled-off pancreatic necrosis: results from a multicenter U. The submucosal tunnel creates a flap that acts as a seal to prevent mediastinal contamination and could be subsequently closed with tissue-approximating units at the finish of the procedure. Forty-eight hours after her procedure she was discharged to residence and in a place to consume oral intake. These photographs depict a nonsurvival porcine experiment to reveal the feasibility of transesophageal biopsy of thoracic vertebrae. Note that with this platform counter-traction can be applied while the second arm carries out the dissection. Evaluation of a new multitasking platform for endoscopic full thickness resection. Transgastric natural-orifice transluminal endoscopic surgery peritoneoscopy in people: a pilot research in efficacy and gastrotomy web site choice by using a hybrid method. Transgastric peritoneoscopy and appendectomy: ideas on our first expertise in people. A novel device for compression anastomosis that makes use of self-assembling magnets allows for transoral creation of immediate and large-caliber gastrojejunostomy in a porcine model. Endoscopic closure of duodenal perforations by utilizing an over-the-scope clip: a randomized, controlled porcine study. Comparison of gastrotomy closure modalities for natural orifice translumenal surgical procedure: a canine research. This system is capable of the position of interrupted or running sutures without tying a knot. The diagrams show the suturing approach: (b) OverStitch suturing system is mounted on the double-channel endoscope; (c) magnified view of the working portion of the suturing system frontloaded to the tip of the endoscope; (d) needle puncturing the gastric wall above the fistula; (e) a needle and thread are passed by way of the gastric wall above and under the fistula; (f) the needle is released out of the suturing device to serve as a tissue anchor, and a cinching mechanism is superior into the stomach; (g) the thread is tightened, closing the fistula, then the cinching mechanism is deployed completing the sew. Endoscopic sleeve gastroplasty: a potential endoscopic various to surgical sleeve gastrectomy for remedy of obesity. Peroral transgastric endoscopic ligation of fallopian tubes with long-term survival in a porcine model. A nonsurvival research was performed in two pregnant sheep and a 3rd sheep was survived. Successful diagnostic and therapeutic intrauterine fetal interventions by pure orifice translumenal endoscopic surgical procedure (with videos). Entry into the peritoneal cavity throughout a resection of rectosigmoid lesions has been described with safe closure obtained. A main concern in any transcolonic approach is the danger of infectious antagonistic events. To decrease these risks, a submucosal endoscopic method with a mucosal flap can be utilized. Herein are endoscopic footage of transcolonic peritoneoscopy with submucosal endoscopy with mucosal flap in a porcine survival model. Transcolonic peritoneoscopy through the use of submucosal endoscopy with mucosal flap for the detection of peritoneal bead concentrating on in the porcine survival mannequin: a feasibility and effectiveness study. Double-contrast radiography is a useful technique for diagnosing a large spectrum of pathological processes within the gastrointestinal tract. In some instances, barium research could demonstrate abnormalities that are missed or misinterpreted at endoscopic examination. Double-contrast radiography and endoscopy should be thought of as complementary procedures for evaluating suspected gastrointestinal disease. Close-up view of supine plain radiograph of the abdomen exhibits tiny, mottled and linear collections of gas within the wall of the descending colon. More inferiorly, pyriform sinuses (P) type the anterior portion of lateral food channels. The arcuate line (long white arrows) is attributable to regular laryngeal impression on the collapsed hypopharynx. In this case, both true (T) and false (F) vocal cords are outlined with aspirated barium within the larynx. Redundant mucosal folds overlie the muscular means of the arytenoid (curved white arrow) and cricoid (curved black arrow) cartilages. Aspirated barium outlines the laryngeal vestibule (short white arrow) and ventricle. Deformity of the larger curvature (black arrow) is depicted adjacent to the ulcer. Tight, constricted section (white arrow) and distal mass effect (black arrows) are seen. One metastasis causes spiculation and fixation of the small bowel wall (white arrow) with normal distensibility of the other wall (small black arrows). Another metastasis appears en face as a filling defect (large black arrows) inflicting distortion of folds. The smaller, more distal lesion appears as a smooth submucosal mass (black arrow). However, a bigger lesion (white arrow) is associated with outward extension into the mesentery. Because of a historical past of systemic lupus erythematosus, these findings were attributed to lupus-related vasculitis. Retroperitoneal air (arrow) is visible alongside the right lateral wall of the pelvis. To work around this, the imager could need to use a special approach (sonographic window) or have the patient change place. Liver Primary indications for liver sonography embrace analysis of diffuse parenchymal disease, focal liver mass, vascular illness, trauma, and transplantation. Parenchymal illnesses similar to fatty liver and cirrhosis have typical sonographic appearances that are useful in confirming the medical prognosis. Hepatic steatosis commonly seems as a diffusely echogenic liver, but fatty infiltration may also seem geographic and focal within the liver. Other masses, nevertheless, are indeterminate and require further imaging or biopsy for analysis. Doppler sonography is the first-line modality in analysis of hepatic vascular disease. This pattern has been referred to because the "starry sky" pattern, and may be seen in hepatitis. Sagittal sonogram of the best hepatic lobe reveals innumerable well-circumscribed anechoic cystic lots in the liver (arrows) in a patient with polycystic liver disease. Sagittal sonogram of the right hepatic lobe shows echogenic liver with coarsened echotexture within the setting of hepatic steatosis. Two small hypoechoic constructions (arrows) alongside the gallbladder fossa symbolize focal fatty sparing. Spectral Doppler interrogation of the thrombus demonstrates an arterial waveform throughout the thrombus. The presence of inner vascularity and arterial waveform differentiates tumor thrombus from bland thrombus. Sagittal sonogram of the proper hepatic lobe reveals a subtle isoechoic mass (between calipers). Color and spectral Doppler of the principle hepatic artery (arrow) show a standard low resistance arterial waveform with normal resistive index of zero. Transverse sonogram of the proper hepatic lobe exhibits innumerable masses with isoechoic facilities and thick peripheral hyperechoic halos (arrows), suitable with metastatic illness. Color Doppler picture of the primary hepatic artery (arrow) exhibits an enlarged and tortuous primary hepatic artery to provide blood circulate to the liver within the setting of portal vein thrombosis. The giant tortuous major hepatic artery can be referred to as a "corkscrew" hepatic artery.
The femoral nerve (see cutaway) is buried within the substance of the psoas major and emerges from the muscle just above where it crosses under the inguinal ligament erectile dysfunction drugs at cvs cialis soft 20 mg discount with visa. The white line erectile dysfunction weight loss generic cialis soft 40 mg mastercard, or arcus tendineus erectile dysfunction diabetes viagra cialis soft 40 mg safe, stretches between the ischial backbone and the lower margin of the pubic bone. The levator ani takes its origin from the thickened obturator internus fascia (the arcus tendineus), in addition to from the decrease margin of the pubic ramus. The inside iliac, or hypogastric, vessels supply the pelvic viscera through a number of branches and tributaries. The hypogastric artery divides into a superior posterior division and an inferior anterior division. From the posterior division, the following emanate: superior gluteal vessels, lateral sacral vessels, and iliolumbar vessels. Anterior division branches include lateral umbilical, superior and inferior vesical, obturator, uterine, and vaginal. Terminal branches of the anterior division embrace the inferior gluteal and internal pudendal vessels. The posterior division of the hypogastric artery will lead the dissector to the sacral nerve roots and the sciatic nerve. The obturator neurovascular bundle is greatest exposed by retraction of the exterior iliac vein. The lateral umbilical vessels ascend the anterior stomach wall supported superficial to the exterior iliac vessels on both side of the urachus (not shown here). After bifurcating from the common iliac artery, the hypogastric artery (internal iliac artery) itself immediately splits into anterior and posterior divisions. The posterior division branches to type the superior gluteal, lateral sacral, and iliolumbar vessels. Following the posterior division down into the depths of the pelvis will result in the sacral nerve roots, which collectively constitute the massive sciatic nerve. When the fats is cleared from this space, the lateral margins of the fossa are seen and consist of the pubic bone and the obturator internus muscle. Several branches of the anterior division of the hypogastric artery can also be identified. These embody the lateral umbilical vessels, the superior vesical vessels, and the obturator vessels. The terminal branches of the anterior division are the inner pudendal and inferior gluteal vessels. The inside pudendal artery really leaves the pelvis via the larger sciatic foramen then reenters by crossing behind and underneath the sacrospinous ligament to reenter the pelvis through the lesser sciatic foramen. The relationship of the sacrospinous and sacrotuberous ligaments to major pelvic vessels and nerves is of necessary scientific value in that surgical procedure performed in this space should be exact to keep away from damage to those very important constructions. Because some urethral tape-suspensory surgical procedures use the obturator foramen, the exact location of the obturator vessels and nerves is required to keep away from injury to these constructions. Exposure of the pelvic ureter is a required talent for anatomists as well as for gynecologic surgeons. Any method to accomplish the aim of ureteral identification ought to be easily performed with a low risk for bleeding or ureteral injury. On the proper aspect, the surgeon or anatomist should grasp the cecum, elevate it, and place gentle traction toward the left. As the cecum is freed, the psoas main muscle comes into view, as do the proper ureter and customary iliac vessels. The ureter could be easily separated from the peritoneal edge with a dissecting scissors, using a closed-push, open-spread technique. The ovarian pedicle and the ureter ought to be separated from one another by sharp dissection. Only after both structures are individually recognized should the ovarian vessels be clamped, reduce, and ligated. If short-cuts are taken in precisely figuring out and securing the anatomic landmarks, ureteral harm will be inevitable. The left ureter is recognized by comparable measures to those described for the right side of the pelvis. However, on the left, the sigmoid colon is grasped and pulled to the best, thereby inserting rigidity on the left peritoneal attachment. Once this is done and the free areolar tissue dissected, the psoas major muscle comes immediately into view. The left ureter proceeds deep into the pelvis to the left and within the bed of the sigmoid colon. As the proper and left ureters descend inferiorly and caudally into the depths of the pelvis, additionally they vector medially. This dissection is sharply carried out and requires knowledge of the sense of direction that the ureter is taking via the cardinal ligament. A tonsil clamp creates an oblique tunnel over (superiorly and anteriorly) the ureter. Note the interior pudendal artery and the pudendal nerve leaving the pelvis via the superior sacrosciatic foramen and reentering by way of the inferior sacrosciatic foramen. Note that the femoral nerve (within the substance of the psoas major muscle) emerges from throughout the psoas main muscle as it passes exposed beneath the inguinal ligament. The large sciatic nerve (L4, L5, S1, S2, S3) leaves the pelvis over the piriformis muscle through the larger sacrosciatic foramen. Note that the sacrospinous and sacrotuberous ligaments form the sciatic foramina from the sacrosciatic notches. The peritoneum (parietal) supporting the cecum to the right abdominal gutter is minimize (dashed line). The underlying psoas main muscle, common iliac vessels, and ureter are introduced into clear view. The proper frequent iliac vessels, the vena cava, and the ureter are introduced into view. The uterine vessels are shown crossing the ureter at the level of the cardinal ligament. Note the best ovarian vessels cut and ligated however overlying the ureter on the proper side. This view is oriented to allow remark of the field from above, wanting caudally. The lateral peritoneal attachments of the sigmoid and descending colon are minimize along the left gutter (dashed line in inset), allowing free mobilization of the big bowel. The left ovarian vessels, which overlie the ureter, have been eliminated on this drawing. The ovarian vessels have been pulled laterally to separate them from the ureters and to higher expose the ureters. The cardinal ligaments have been exposed by incising the posterior leaf of the broad ligament. Note the uterine vessels above and the vaginal vessels under because the ureters curve inward during their brief journey through the cardinal ligaments. The infundibulopelvic ligament (ovarian vessels) has been retracted laterally and away from the ureters on this picture. In precise dissection, the ovarian vessels and the ureters cross over the common iliac vessels very near each other. The dashed line exhibits how an incision might be made via the highest of the ligament and extended to open the anterior and posterior leaves. The free areolar tissues between the leaves have been dissected to expose the deeply located left ureter. Tonsil clamps are positioned on the uterine artery to divide it above the purpose where the ureter crosses under it. The uterine artery is a significant branch of the anterior division of the hypogastric artery. The uterine artery in the neighborhood of the junction of the cervix and uterine body splits into ascending and descending branches. The former is a coiled vessel that makes its means up the facet of the uterus beneath the round ligament to the area between the junction of the tube, utero-ovarian ligament, and higher uterine corpus.
Diseases
Cornual Anastomosis the fimbriated finish of the tube is probed by the use of a polyethylene cannula inserted into the tube erectile dysfunction caused by lack of sleep 40 mg cialis soft cheap with mastercard. The tube is injected with 1: 200 vasopressin and is minimize just proximal to the obstruction erectile dysfunction journal articles cialis soft 40 mg with mastercard. When the open portion of the interstitial portion of the oviduct is transected impotence bicycle seat 40 mg cialis soft discount otc, blue dye squirts forth. A lacrimal probe is inserted into the interstitial tube lumen and is superior into the uterine cavity. The serosal portion of the oviduct then is anchored to the uterine serosa with 5-0 Vicryl. Typically, this operation is performed on the time of cesarean part, or immediately postpartum within the case of vaginal supply. Modified Irving and Pomeroy strategies are enhanced because further tubal separation may be anticipated as the end result of fast regression of the uterine mass to a nonpregnant measurement and shape. Simple fimbriectomy or ampullary-isthmus excision is well suited as an interim operation. Whatever methodology is selected for tubal sterilization, sure precepts must be adopted. Paradoxically, sufferers additionally have to be informed that a failure price is related to every operation. Next the tube ought to be traced from the uterus to the fimbriated end after which secured with a Babcock clamp or stay suture-ligature. Finally, the placement of the ipsilateral ovary should be viewed relative to the tube. The proximal and distal ends of the tube are grasped with Babcock clamps, and the stretched tube is held straight and elevated upward in order to clearly expose the mesosalpinx. A needle guide or mosquito clamp is pushed into the posterior facet of the uterus after the gap that the tied proximal tubal segment will stretch with out rigidity is measured. Each needle is sutured through the information via the hole created in the posterior wall of the uterus. As the needle guide is removed, the ends of the suture (after the needles have been cut free) are tightened; the tightened suture secures the proximal tubal stump into the myometrium of the posterior uterine wall. Scissors are used to excise the knuckle of tube by cutting along the superior marginal floor above the Kelly clamp software. Fimbriectomy this operation could additionally be carried out by minilaparotomy (abdominally) or by posterior colpotomy (vaginally) or by laparoscopy. The oviduct is located and secured close to the uterus with a Babcock or Allis clamp. The fimbriated portion of the tube is clamped with a Kelly clamp; a second Kelly clamp is positioned throughout the tube at the ampullary-fimbrial junction. The tube is cut between the primary and second Kelly clamps, and the fimbriated end sent to the pathology laboratory. The segment of tube is cut out and sent to the pathology laboratory for prognosis. Note anteriorly the curving round ligament and under (arrow) the whitish utero-ovarian ligament. Panoramic view from the entrance (anterior) detailing the three tubular buildings emanating from the highest of the uterus (dark line). White blanching (coagulation) happens above and below the point the place the tube is held by the forceps. For passable hemostasis to be achieved, coagulation continues until the mesosalpinx is coagulated. A coagulated section of the oviduct is eliminated and sent to the pathology laboratory. Completed laparoscopic bilateral partial salpingectomy carried out by electrosurgical coagulation. The failure was brought on by bilateral ligation of the round ligaments quite than ligation of the oviducts (arrows). Two mosquito or Kelly clamps are positioned at each extreme of the isolated segment, and the section is reduce out. Suture-ligatures are placed through each end of the remaining oviduct and tied beneath the clamps, that are then eliminated; nonetheless, the double-armed suture connected to the uterine oviductal remnant is held. A grooved director or mosquito clamp is used to burrow a hole into the posterior side of the uterus. The uterine oviductal phase is buried within the uterine wall because the suture ends are pulled snugly and tied into place. A second Kelly clamp is positioned across the bottom of the knuckle, and the tube above the Kelly clamp is minimize off and sent to the pathology laboratory. Next, a zero chromic catgut ligature is placed across the Kelly clamp and is tied snugly into place. As the pregnant uterus involutes and the tensile energy of the chromic catgut weakens, the cut tube segments are pulled apart. The fimbriated ends of the tube are clamped with Kelly clamps, and the fimbriae are amputated. Simple Bilateral Partial Salpingectomy that is an interval operation and may be performed by minilaparotomy or by laparoscopy. A hole is made with a mosquito clamp in the mesosalpinx directly below the elevated portion of the oviduct. Alternatively, the ends of the tube may be coagulated with bipolar forceps somewhat than clamped and ligated with suture. Either pole of the tubal section is clamped with mosquito clamps, and the segment (1. Silastic Band Operation this technique usually is performed by laparoscopy; nevertheless, it might be used at laparotomy as well. This is a tong forceps with two cylindrical tubes by which the outer cylinder moves over the inside cylinder as the tongs grasper pulls a knuckle of tube into the inside cylinder. The tube simply necroses slowly because its blood supply is compromised by the tight Silastic band. Uchida Operation the Uchida operation may be carried out postpartum or as an interval process. With a sharp scalpel, the dorsum (antimesenteric side) of the tube is shallowly incised in a parallel style to the axis of the oviduct. Bilateral partial salpingectomy is performed in precisely the same manner as the Irving operation; nonetheless, neither tubal segment is olated from the other. The Uchida operation uses an injection of 1: 200 vasopressin into the mesosalpinx for the twin purpose of hemostasis and creation of a dissection airplane. A linear incision is made above the oviduct within the ballooned-out phase that has adopted vasopressin injection. With a Uchida clamp or a loosely utilized Allis clamp, the oviduct is free of the mesentery by moving the clamp back and forth throughout the mesosalpinx. The freed phase is ligated at both end with 2-0 silk or nylon, and the section is cut out. The fimbriated finish of the tube remains out of the mesosalpinx during closure of the mesentery, whereas the uterine end of the tube is buried within the mesosalpinx. Note that a Silastic band has been loaded onto the internal cylinder of the forceps at its terminal portion. Next, the tongs containing a knuckle of tube are drawn into the internal cylinder of the tongs forceps. At the same time, the spring-loaded inner cylinder is pulled again in opposition to the mounted outer cylinder, causing the band to be pushed onto the base of the knuckle of oviduct. Note the white color of the banded knuckle of oviduct, which is the outcomes of its blood provide being reduce off. The anterior aspects of the proximal urethra and extraperitoneal parts of the bladder are seen upon exposure of the retropubic area. Note that the floor of the retropubic house is shaped by the fibrofatty internal lining of the vaginal wall, which has historically been termed endopelvic or perivesical fascia, and fibers from the levator ani muscle. More lately it has been realized that this trapezoid construction that gives help to the proximal urethra and bladder is nothing more than the muscular lining of the vaginal wall. Note how the proximal urethra and extraperitoneal parts of the bladder are exposed by way of the retropubic house.

A long retractor is then placed to mobilize the rectum medially erectile dysfunction causes of cialis soft 20 mg discount line, and a notched speculum is inserted by palpation beneath the hook level erectile dysfunction cancer cialis soft 20 mg buy discount on line. For this procedure to be carried out on the right purchase erectile dysfunction drugs 20 mg cialis soft overnight delivery, the suture-capturing device (Capio Needle driver; Boston Scientific Corp, Watertown, Mass. With the tip of the middle finger, the suturecapturing system notch is positioned 2 to three cm medial to the ischial backbone, approximately zero. The handle is released, the system is eliminated with the suture, and the suture is tagged. As previously described, a complete of two or three sutures are passed by way of the ligament. After the sew has been placed within the ligament, one finish of the suture is rethreaded on a free needle, sewn into the total thickness of the fibromuscular layer of the undersurface of the vaginal apex, and tied by a single halfstitch, while the free finish of the suture is held lengthy. With this methodology, both ends of the sutures are passed by way of the vaginal epithelium. When this method is used, a delayed absorbable suture should be used as a end result of the knot remains in the vagina. After the sutures have been introduced out by way of the vagina, the vagina is trimmed if essential, and the higher portion of the vaginal wall is closed with an interrupted or continuous delayed absorbable suture. It is important that the vagina comes into contact with the coccygeus muscle and that no suture bridge exists, especially if delayed absorbable sutures are being used. While these sutures are being tied, it might be helpful to perform a rectal examination to detect any suture bridge. A posterior colpoperineorrhaphy is performed as wanted, and the vagina is filled with moist gauze for twenty-four hours. Unique however serious intraoperative issues can happen after sacrospinous colpopexy. Potential issues of the procedure embrace hemorrhage, nerve injury, and rectal harm. Severe hemorrhage requiring a blood transfusion may result from overzealous dissection superior to the coccygeus muscle or ischial backbone. This can lead to hemorrhage from the inferior gluteal vessels, hypogastric venous plexus, or pudendal vessels. If severe bleeding happens within the area across the coccygeus muscle, preliminary management must be to apply stress with a sponge stick for 5 minutes (by the clock). This anatomic space is difficult to method transabdominally or with selective embolization, so bleeding ought to be managed vaginally, if attainable. Moderate to extreme buttock ache on the aspect by which the sacrospinous suspension was carried out can happen in as much as 15% of sufferers. The buttock ache is sort of at all times self-limiting and will resolve by 6 weeks postoperatively. If the pudendal nerve is injured, postoperative symptoms of unilateral vulvar ache and or numbness will happen while injury to the sacral nerve roots will often result in ache down the again of the leg. In either state of affairs instant reoperation with elimination of the offending suture is really helpful. Technique of passage of a Miya hook via the ligament is visualized, as properly as the technique of retrieval of the suture (inset). If the sutures are handed by way of the vaginal epithelium and tied within the vaginal lumen, then delayed absorbable sutures are used. Note the slight bend near the tip to facilitate suture placement into the coccygeussacrospinous ligament complex. Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography � 2012�2013. Sutures are being tied, approximating the apex of the vagina to the coccygeus-sacrospinous ligament advanced. An Allis clamp has been positioned on the anterior vaginal wall, which is the section of the prolapse most probably to recur. Note the posterior distortion of the anterior section after tying of the sacrospinous sutures. The posterior vaginal wall is opened in the midline as for posterior colporrhaphy, and the rectovaginal areas are dissected extensively to the levator muscles bilaterally. A single, 0 delayed absorbable suture is positioned deeply into the levator muscle and fascia. While eradicating the posterior vaginal flap, one should avoid coming into the peritoneum. If the peritoneum is inadvertently entered, the defect should be closed with an interrupted delayed absorbable suture. Absolute hemostasis is necessary to avoid a postoperative hematoma within the vaginal canal. Postoperatively, the patient is mobilized early; nevertheless, heavy lifting is averted for at least 2 months to stop recurrence of the prolapse secondary to breakdown of the repair. The operation is carried out by utterly excising the vaginal mucosa from the underlying vaginal or endopelvic fascia. Similar to the LeFort procedure, bladder neck plication and perineorrhaphy with levatorplasty are often carried out with a colpectomy. Note within the inset that the dissection has been extended laterally on the stage of the proximal urethra to perform a Kelly-Kennedy plication within the hope of providing preferential help to the bladder neck and thus stopping any occult or potential stress incontinence. A portion of the posterior vaginal wall will normally lie over an enterocele, and the surgeon ought to attempt to avoid entering the peritoneal cavity if at all potential. The cut fringe of the anterior incision, at the degree of the cervix, is sewn to the distal reduce edge of the posterior incision with interrupted 2-0 delayed absorbable sutures (inset). Once the cervix is inverted, the interrupted sutures are taken by way of the minimize edges of the lateral portions of the incision on both sides. Once the whole vagina has been inverted, the superior and inferior margins over the rectangle could be sutured horizontally, thus completely obliterating the midportion of the vagina (inset). Draining channels are left in the lateral parts of the vagina to facilitate drainage of any cervical discharge. A levatoroplasty is usually performed to increase posterior pelvic muscle support and narrow the introitus. The vagina is circumscribed by an incision at the web site of the hymen and is marked into quadrants. Purse string sutures are tied 1 before 2 and 2 before three, with progressive invasion of the gentle tissue before tying of every suture. The first quadrant of the vagina over the prolapse is sharply removed from the underlying tissue. The first purse string suture has been tied, and the second purse string suture has been placed. Although stomach sacral colpopexy with artificial mesh is a wellaccepted and proven process, a variety of vaginal procedures with synthetic and biologic mesh have been described and advocated in sure ladies with prolapse. Wide adoption of vaginal mesh use occurred between 2005 and 2010 mostly due to the advertising of commercially out there mesh kits. Consequently, in 2008, after greater than 1000 voluntary reports of security problems in the manufacture and person facility gadget expertise database, the U. The results of those studies will most likely decide the long-term availability and utilization of vaginal mesh kits sooner or later. This chapter critiques the assorted artificial and biologic materials which would possibly be currently obtainable for vaginal augmentation and discusses the technical features of performing a selection of mesh augmented vaginal repairs. A variety of biologic tissue is out there for utilization, together with autologous grafts, allografts, and xenografts. A biologic graft can be used to facilitate anterior and posterior vaginal wall help. When performing an anterior vaginal wall augmentation, one must determine the websites during which the augmented material is going to be fixed to the pelvic flooring. To actually recreate regular support, one should dissect out into the paravaginal house to determine the realm of the obturator internus fascia or arcus tendineus fascia pelvis (white line) because that is the origin of the fibromuscular layer of the vaginal wall that would usually assist the anterior vaginal wall. I would all the time recommend some kind of apical suspension if attainable in conjunction with the graft augmented anterior repair. The mesh is mounted in place within the anterior phase; the trapezoid idea is demonstrated, exhibiting how the mesh creates paravaginal, midline, and transverse assist.
The adverse aspect of utilizing mixed remedy with two antibodies apparently consists of extra antagonistic effects erectile dysfunction and zantac buy 20 mg cialis soft visa. Ipilimumab with gp100 peptide improves overall survival of sufferers with previously treated metastatic melanoma (Hodi et al erectile dysfunction age 35 cheap 20 mg cialis soft mastercard. Adverse events could be long-lasting erectile dysfunction drugs nz cialis soft 20 mg buy line, but most are reversible with acceptable remedy. This receptor plays an essential position in controlling the immune system to prevent inadvertent immune cell activation and autoimmune illness. Traditional chemotherapies and focused anticancer therapies exert their effects by direct cytotoxicity or by tumor growth inhibition. In distinction, nivolumab acts by blocking a adverse regulator of T cell activation and response (Pardoll, 2012). This is a technique that the physique regulates the immune system to avoid an overreaction. Adverse results of utilizing nivolumab embrace fatigue, diarrhea, pruritus, rash, and decreased urge for food. The manageable antagonistic side effects can be lowered by immunomodulatory medicine, though they inflict their very own unwanted effects. This function of pembrolizumab has raised its effectiveness as the immunotherapy of choice for most patients with superior melanoma (Sosman, 2015). The European Commission has permitted using pembrolizumab in patients with superior melanoma, unresectable (metastatic) melanoma, and folks who are previously treated or untreated. This drug has additionally received approval for use within the United States, but just for previously handled patients with advanced melanoma. The antagonistic reactions of pembrolizumab embrace diarrhea, fatigue, nausea, pruritus (itching), rash, and arthralgia (pain in a joint), leucopenia, neutropenia (abnormally small number of white blood cells), and anemia. According to these authors, this therapy resulted in a high fee of sustained tumor regression, with mainly grade 1 or 2 poisonous results. Two such antibodies, tremelimumab and ipilimumab present these effects (Eggermont et al. An adjuvant remedy to improve supply to the mind by way of efflux inhibition could also be a viable choice for improving survival. Oral coadministration of elacridar strongly increased oral availability and mind penetration of vemurafenib in wild-type mice, especially on the clinically extra related larger vemurafenib dose (25 mg/kg). This synergism from the mix leads to the 75% radiologic response, symptomatic aid in 45%, and a median survival of 13. This methodology generates systemic T cell responses that may target distant metastases beyond the initially handled tumor mass. Promising preclinical outcomes and some initial success in medical trials have been obtained (Singh and Overwijk, 2015). During the final three a long time a lot of therapeutic agents, together with trastuzumab, bevacizumab, pertuzumab, ipilimumab, sorafenib, capecitabine, gemcitabine, lapatinib, vinorelbine, tamoxifen, iniparib, docetaxel, everolimus, eribulin, tanespimycin, and bonemodifying agents, have been used alone or in combination towards breast most cancers with variable effectiveness and side effects. Poor (nonuniform) growth of vasculature throughout a solid tumor is liable for inconsistent focus of oxygen, which leads to a significant level of intra- and intertumor heterogeneity. Disease-free interval performs an essential position in the prognosis for sufferers with relapsed breast most cancers. This difference within the total survival of sufferers in these two studies could also be defined in part whether or not or not surgical procedure of the primary tumor was used. Treatment Chemotherapeutic agents and antibodies, which have been used for sufferers with breast cancer, are summarized beneath. This examine reveals response evaluation criteria in solid tumors-defined responses for 17-demethoxygeldanamycin in solid tumors. Trastuzumab resistance is linked to the activation of phosphoinositol 3-kinase (p13K) pathway. Lapatinib extended the time to progression and increased the speed of response to capecitabine in sufferers who had received anthracycline-based and taxanebased chemotherapy, and whose tumors had progressed on trastuzumab. It is also important to characterize mechanisms of resistance in metastatic tumors. Treatment of early stage breast most cancers reduces the chance of illness recurrence and prolongs overall survival. However, this routine might accompany toxicity to coronary heart, particularly within the form of left ventricular dysfunction. This mixture improved medical profit in terms of increased progression-free survival in first-line therapy of metastatic breast cancer (Robert et al. Bevacizumab mixed with generally used chemotherapies (capecitabine, gemcitabine, or vinorelbine). This combination improved medical benefit in terms of increased progression-free survival (Brufsky et al. This antibody is well tolerated in closely pretreated sufferers with breast most cancers (Yardley et al. This antibody is conjugated to potent cytotoxin monomethyl auristatin E, and is restricted to this glycoprotein. Despite the absence of a response reported, a small scientific profit fee of 19% was noticed in metastatic breast most cancers (Rudek et al. This mixture increased scientific profit rate, time to development, and overall survival compared with tamoxifen alone in postmenopausal girls with aromatase resistance metastatic breast most cancers (Bachelot et al. Eribulin has acquired a minimal of two chemotherapeutic regimens for the remedy of metastatic breast most cancers. These agents are recommended for sufferers with metastatic breast most cancers with proof of bone destruction (Van Poznak et al. All sufferers ought to have a dental examination and preventive dentistry before using these agents. Eating nonstarchy vegetables, fruits, and meals containing beta-carotene and/or vitamin C protects in opposition to this cancer, and meat most likely will increase the risk of this illness. In distinction, the incidence of brain metastasis is greater when the histological sort is adenocarcinoma. Similar sample is seen in patients with nonsmall cell lung carcinoma, where the incidence of brain metastasis is greater in sufferers with adenocarcinoma versus squamous cell carcinoma (Mujoomdar et al. There is a comparatively quick interval between the diagnosis of the primary esophageal tumor and improvement of brain metastasis (Smith and Miller, 2011). To reduce this downside, a neurosurgical procedure can be used to obtain a definitive analysis and an effective treatment (Spallone and Izzo, 2013). Well-differentiated adenocarcinomas are hypointense, whereas small and huge cell neuroendocrine tumors present hyperintensity (Hayashida et al. The length of life and the quality of life are the 2 most necessary measures of most cancers care, and the remedy should fulfill these necessities. Cancer sufferers must be defined all out there remedy options, and the ultimate decision for treatment needs to be made in session with a wellinformed patient. Endoscopic ultrasonography is often used to decide the depth of tumor invasion. At analysis sufferers are initially staged for local development or systemic spread (metastasis) of their illness, each of which determine whether or not a curative therapeutic approach ought to be thought-about. Surgical resection of brain metastases can significantly decrease morbidity and prolong survival as compared to nonsurgical approaches (Patel et al. Generally, surgical excision is most well-liked in instances with a solitary lesion or adjacent a number of metastases, instances with diagnostic uncertainty, or instances with life-threatening and critically positioned metastases (Agrawal et al. In fact, within the majority of cases, complete surgical resection of the first tumor is the key to attempting healing remedy (Lemke et al. However, typically this remedy is insufficient because the most cancers already has metastasized, and due to this fact, subsequent adjuvant therapy is required. The affected person initially responded properly with regard to liver metastasis, however subsequently developed a number of mind metastases. The medical research by these authors indicated the next median survival with respect to the remedy modality: Surgery: 7 months Radiation remedy: 4 months Chemotherapy: 1. However, some evidence is out there indicating that aggressive therapy, together with surgical resection may extend survival in selected patients, particularly those who are identified with solitary brain metastasis illness (Lemke et al. Both sufferers underwent complete gastrectomy, center to lower esophagectomy, and Roux-en Y reconstruction using the jejunum.
The possibility that other adenomas and even cancers are current in this colon emphasizes the necessity to erectile dysfunction pump rings generic cialis soft 40 mg line perform colonoscopy at the time of diagnosis to clear the colon of different lesions that could alter affected person administration top rated erectile dysfunction pills cheap 20 mg cialis soft otc. This is a function that nearly all authors believe ought to prompt resection following a diagnosis of "most cancers in a polyp erectile dysfunction workup 20 mg cialis soft trusted. It lacks typical dysplasia but is totally able to progressing to invasive carcinoma. There is serrated structure of the epithelial cells in addition to conventional epithelial dysplasia like that of an strange adenoma. Aberrant ganglion cells and Schwann cells (bland spindled cells) proliferate within the colonic lamina propria. This lesion shows differentiation alongside sweat gland lineage and is found in the perineum of females. In basic, aging could be slowed down by not smoking or chewing tobacco, by preventing or minimizing perpetual stress (anger, extreme competition), by abstinence from alcoholic beverages, by having common train and sleep, and by having a healthy diet. There is little question that regular physical activity is related to a decreased risk of mortality, and contributes to the first and secondary prevention or delay of many kinds of ailments, together with most cancers. Perpetual stress also performs a component within the development of cancer and different diseases. Although anyone can develop most cancers, the danger of developing most cancers increases substantially with age. The frequency of cancer varies by geographic areas, especially in developed international locations versus developing countries. Cancer is a significant public well being drawback worldwide, and is anticipated to surpass cardiovascular diseases as the main explanation for dying in the next few years. Estimated new major cancer instances and deaths in the United States in 2015 are (Siegel et al. Cancer needs to be diagnosed at an early stage, or even before cells turn out to be cancerous (removal of precancerous lesions) when it might be treatable. In order to understand brain metastasis from main most cancers, we need to comprehend how cancer cells escape from the first tumor site, intravasate into blood vessels, accumulate in mind capillaries, survive the hematogenous dissemination to the mind, extravasate and proliferate and develop angiogenic capacity to establish mind metastases. Metastatic colonization is strongly influenced by the interaction of main most cancers cells with host cells present or recruited to the microenvironment right into a structure known as the metastatic area of interest (Ord��ez-Mor�n and Huelsken, 2014). This native surroundings is responsible not only for the preliminary metastatic colonization of the host tissue but additionally for the development of the illness. To succeed in discovering an effective use of therapeutic drugs, we should also understand higher the immunologically distinct space that excludes drug macromolecules from the mind. It is estimated that 100,000�170,000 persons are inflicted by metastatic mind cancer per year within the United States. Generally, intracranial metastatic lesions are extra common than primary tumors of the brain (Gavrilovic and Posner, 2005). Metastatic brain tumors are 10 occasions extra frequent than primary brain tumors, and symbolize 20�40% of all intracranial neoplasms in adults (Go et al. Approximately, 10�20% of all brain metastases are single tumors, and the remaining are a number of tumors. Lung, breast, colon, and kidney cancers and melanoma generally unfold to the brain. Breast and kidney cancers usually cause single mind tumors, while lung most cancers and melanoma are probably to trigger a quantity of mind tumors. Approximately, 85% of metastatic lesions are positioned within the cerebrum, while the remaining are located within the cerebellum. Autopsy analyses have shown that the incidence of mind metastases is as excessive as 30% in sufferers with breast cancer, 40% in these with lung most cancers, 75% in those with melanoma, and 6% with those with kidney or bladder cancer. Brain metastases are among the many most devastating and debilitating problems of lung most cancers, breast most cancers, unknown most cancers, and melanoma. Patients with brain metastases typically develop critical deterioration in neurological and neurocognitive capabilities. Intracranial bleeding is likely one of the fatal issues encountered in the patients. Neurosurgery is used for patients with a few metastatic lesions offered the lesions are surgically accessible and the affected person can tolerate the operation. Surgical resection could instantly remove life-threatening or symptom-generating mass effect and remove the supply of perifocal edema. To reduce the risk of tumor recurrence and leptomeningeal spread "en bloc" strategy quite than piecemeal technique has been used. Some research have demonstrated superior outcomes, whereas another research report adverse influence on neurorecognition (Brown et al. Use of immunotherapy for patients with mind metastasis can additionally be discussed in this quantity and by Powell and Dudek (2009). Primary tumor ulceration is the strongest predictor of brain metastases improvement, and remains an independent predictor of decreased brain metastasis survival after treatment (Zakrzewski et al. The data relating to the biology of ulceration and molecular mechanisms underlying its opposed impression on clinical consequence is equally necessary. Admittedly, outcomes of ordinary therapies mentioned above have been less than spectacular. Recently launched therapies, together with multidisciplinary approach, could result in encouraging constructive treatment outcomes. However, the incidence of each of these cancer types has been increasing in the course of the past many years. It is estimated that one in every three most cancers varieties identified is a pores and skin most cancers, and one in each five Americans will develop pores and skin most cancers in their lifetime. For example, the incidence of melanoma increased from 15/100,000 persons in 1986 to more than 25/100,000 persons in 2006 in the United States. Melanoma is a malignant neoplasm that occurs principally in adults, and may originate de novo from a pigmented naevi (a benign localized overgrowth of melanin-forming cells of the skin). It can also start in different pigmented tissues corresponding to in the eye or the intestines. The most aggressive kind of pores and skin cancer, melanomas usually grow in densely packed mobile "nests" that contain minimal extracellular matrix (fibronectin, collagen, or laminin). This pitfall is especially widespread within the prognosis of rare and weird melanoma variants and melanoma resembling those in typical melanoma. These features embrace irregular functional components with pagetoid spread, melanocyte atypia, lack of dermal maturation, dermal mitotic activity, intense melanin pigmentation, a desmoplastic stromal response, and dermal regression. We want improved understanding of the molecular drivers and heterogeneity of this disease. The frequency of metastasis is estimated to be 40% or much more in melanoma patients (Soffietti et al. Tumor-related inflammation is associated with upregulation of proinflammation cytokines, which is associated with ulceration. Approximately, 75% of patients with metastatic melanoma develop mind metastases in the course of the course of their disease. Melanoma is the third commonest analysis amongst sufferers with mind metastases, after lung and breast cancer. Brain metastasis is a serious explanation for demise in melanoma sufferers, the frequency of which is on the rise. However, regardless of these poor outcomes, approximately 5% of patients with mind metastases from melanoma are long-term survivors. The identification of factors that may predict outcomes could profit the medical administration of these sufferers. Other components concerned are less than three parenchymal metastases, leptomeningeal involvement, and the development of brain metastases after prior systemic therapies. A solitary brain lesion, surgical therapy, and an excellent Karnofsky Performance Status point out an excellent prognosis (Celix and Silbergeld, 2014). Recent developments in melanoma remedy have influenced the administration of metastatic melanoma patients. An essential prerequisite to obtain this aim is to establish molecules expressed by brain-metastasizing melanoma cells, which are involved within the focused migration of such cells to the brain (Klein et al. These molecules maintain melanoma cell survival and promote their propagation in the mind. The improvement of an efficient therapy against mind metastasis will be helped by understanding the interactions of those molecules with the microenvironment of the mind tissue.






