Prevacid
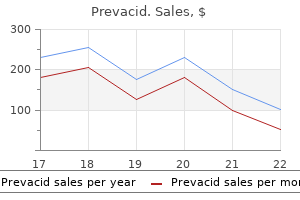
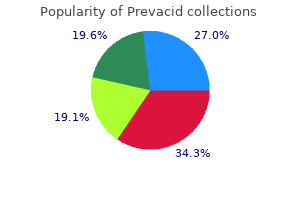
Prevacid
Prevacid dosages: 30 mg, 15 mg
Prevacid packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Although many options are held in common with rheumatoid arthritis, the shortage of seropositivity for rheumatoid factor led to the designation seronegative spondyloarthropathies gastritis symptoms itching prevacid 30 mg buy without prescription. Even though an association between the gene and illness is understood, the precise mechanism by which illness develops remains unknown gastritis management buy discount prevacid 15 mg. Significant dysfunction and progressive disability are the norm, though a large percentage of patients are in a place to maintain employment and productiveness gastritis diet ����� buy discount prevacid 30 mg on-line. As could be expected, individuals with bodily demanding occupations and decrease instructional status are at greater risk for work incapacity. Derived from Greek, the name refers to an inflammatory situation of the backbone (spondylos) resulting in stiffening and angulation (angkylos). Even although males are more commonly affected (3: 1 ratio), women carry a higher risk of having an affected baby. In fact, the arthropathy could precede the symptoms of bowel illness by a decade or extra. When current, peripheral symptoms often follow the course and severity of the underlying bowel illness. However, patients with enteropathic arthritis more generally have peripheral joint involvement (10% to 20%), followed by sacroiliitis (10%) and spondylitis (3% to 4%). At least 40% of patients with psoriasis are found to have radiographic evidence of inflammatory arthritis,8 and vital disability might develop in sufferers with psoriatic arthritis, with up to 20% demonstrating a rapidly progressive, debilitating medical course. Psoriatic arthritis may be associated with weight problems, hypertension, dyslipidemia, and insulin resistance because of the shared inflammatory pathway. Bacteria related to such diseases embrace enteric and venereal pathogens corresponding to Shigella, Salmonella, and Chlamydia species. It also tends to be discontinuous in its radiographic look, with affected areas being noted to be spaced between normal-appearing areas. Urethritis often develops first, sometimes 2 to 4 weeks after an infection, followed by conjunctivitis and later arthritis. The prevalence of the gene is 8% within the general white inhabitants and 4% in the African American population. This danger will increase to approximately 20% to 30% when a first-degree relative carries the prognosis. Ossification is observed at such sites, in addition to on the degree of the annulus fibrosus and zygapophyseal joints, and leads to progressive ankylosis. Ossification also occurs in heterotopic places, such as throughout the hip musculature after complete hip arthroplasty. Extraskeletal manifestations include involvement of the eyes, pores and skin, and cardiovascular system. Fever, weight loss, and systemic symptoms could also be seen in periods of active disease. The spondyloarthropathies have somewhat variable medical findings, depending on the subtype. A mixture of history and findings on bodily examination, together with imaging and laboratory checks, is used within the analysis of those conditions. Although advanced illness may have obvious hallmarks, early disease could also be delicate. Inflammatory again pain-characterized by age < forty at onset, insidious onset, symptoms for >3 mo, association with morning stiffness, and improvement with train 2. Asymmetrical synovitis, predominantly of the lower limbs-soft tissue swelling, joint effusion and warmth, and reductions in each active and passive vary of movement. Symptoms are worse after a interval of rest Once the entry standards are glad, the next are investigated: 1. Symptoms related to enthesopathy embody significant plantar fasciitis, again worse within the morning and after a interval of relaxation. The Achilles tendon, fifth metatarsal, tibial tuberosity, patella, larger femoral trochanter, iliac crest, and ischial tuberosity are additionally widespread sites. Patients with spinal deformity will typically have had disease for a decade or more. Such patients complain of issue maintaining forward gaze (horizontal gaze) while strolling and observe difficulty especially when going up an incline or stairs. Although kyphotic sagittal imbalance is typical, coronal airplane deformity might happen as nicely. Advanced deformity with a chin-on-chest appearance creates issues related to hygiene as a end result of patients are unable to entry their anterior neck skin folds. On physical examination, patients are famous to have stiffness, muscular atrophy, and probably a kyphotic posture (depending on the stage of the disease). It is performed by marking a 15-cm length of pores and skin extending from 10 cm above the lumbosacral junction to 5 cm under. Patients with kyphosis try to revive sagittal stability by way of hip extension, knee flexion, and ankle plantar flexion. As a hip flexion contracture develops, patients adopt a forward-flexed posture that may exaggerate the looks of the kyphosis. Evaluation of the hips is crucial in arriving at an correct evaluation of the diploma of spinal deformity that might be present. Extraskeletal disease involves multiple organ systems, with each subtype of spondyloarthropathy having a considerably different predilection for every. Such illness contains heart problems, extra particularly aortic insufficiency and conduction disturbances; pulmonary disease, similar to apical pulmonary fibrosis; deposition illness, similar to amyloidosis with its related renal dysfunction; and neurological illness corresponding to encephalitis, transverse myelitis, and peripheral neuropathy. Because the higher cervical backbone tends to lag behind in bony ankylosis, compensatory hypermobility might develop and lead to neurological complications. Cauda equina syndrome could also be seen, perhaps as a end result of persistent irritation, demyelination, and fibrosis, along with the event of arachnoid diverticula. As marginal syndesmophytes form alongside the intervertebral disks, the backbone takes on the appearance of a single lengthy bone (contributing to the lack of flexibility and elevated danger for fracture). These spinal changes usually begin distally within the lumbar spine and progress slowly cephalad. Note the bridging syndesmophytes (long arrow) and fused zygapophyseal joints (short arrow). Earlier in the illness, erosions are noted at the lower finish of the joint, particularly over the iliac side. As ossification progresses along entheses such as the iliac crests, ischial tuberosities, and femoral trochanters, a process generally known as "whiskering" is noticed. Spondylodiskitis is characterized by an inflammatory, erosive process of the intervertebral disk, commonly at the thoracolumbar junction. It is unknown whether this erosion represents an space of persistent irritation, failure of ankylosis across an area of high mechanical stress, or an area of nonunion after trauma to the already ankylosed backbone. Methods specific to enthesitis that focus on the ligamentous and muscular insertions on the stage of the Achilles tendon, femur, and humerus have been used. This is noted on plain x-ray imaging research, but dual-energy x-ray absorptiometry could present a paradoxical enhance in density on account of enthesopathy and greater peripheral bone formation. Patients who often carry out back workout routines and have acceptable social assist have been proven to have a higher degree of perform. This index supplies sufferers a score from zero to a hundred, with greater scores indicating higher incapacity. Muscle relaxants may be used at the facet of other drugs to ease the muscle spasms that accompany the spinal illness. Sulfasalazine and methotrexate have a historical past of efficient use in sufferers with rheumatoid arthritis and are used for remedy of the spondyloarthropathies as well. Nevertheless, their efficacy in treating axial spinal pathology such as seen within the spondyloarthropathies is relatively limited. However, the risk for critical infection will increase significantly with such remedy. Widespread use of those drugs is limited somewhat by cost54,55 and concerns concerning long-term use. This sometimes requires constructing pillows behind their neck and thoracic spine and even elevating the top of the mattress for a thoracolumbar injury.
Corrections are required to account for the distinction in density between air, bone, brain, and other tissues gastritis diet king prevacid 30 mg purchase free shipping. To reduce uncertainty, ports are preferentially selected in order that they penetrate bone perpendicular to the surface and avoid heterogeneous regions such as sinuses, mastoids, ears, and the bottom of the skull, which can introduce small errors in dosimetry calculations gastritis diet 101 prevacid 15 mg buy cheap line. In 1985, conformal collimation was fully applied, with digitized collimation being transferred to an automated milling machine to create the absolutely conformal apertures gastritis video 30 mg prevacid amex. A new patient positioner was designed to particularly accommodate the fixed horizontal beam line. The new positioner enabled treatment of cranial targets from any course in the superior hemisphere of the pinnacle. Local anesthesia was applied to the contact sites for placement of the fixation pins. Therefore, it was necessary that the beams be aimed via uniform paths to minimize uncertainty. Treatment instances were forty five to 90 minutes from the time of patient entry into the room to the time of exit. Hospital-BasedProtonTherapyFacility Loma Linda University Medical Center was the primary hospitalbased proton facility; it was opened in 1990 and is a middle with proton radiosurgery functionality. Of curiosity, of the following new proton services opened in the United States, none are currently working towards radiosurgery. Locating proton remedy services on major hospital campuses supplies much better entry for patients and is particularly helpful for coordination with different medical care. The gantry rooms use nonisocentric four-axis robotic affected person positioners and amorphous silicon panels for digital imaging quite than film. Final proton beam shaping is achieved with custom brass apertures for every therapy beam and Lucite compensators to create the distal form of the beam. The range and modulation are managed by a binary set of Lexan and lead absorbers somewhat than a modulation wheel. The beam is transported from the cyclotron at 185 MeV and reduced to the mandatory power and depth with the suitable combination of absorbers in the type of a single scattering system. A noninvasive system for immobilization has been developed that comes with the present fiducial marker system that relied on patient anatomy and implanted hardware for alignment rather than an external frame. The first proton therapy planning system approved by the Food and Drug Administration was introduced in 1998. It makes use of a pencil beam dose algorithm to mannequin scatter somewhat than using generic dose matches. Trends are shifting toward emphasizing cost-effectiveness, compactness, ease of use, safety, good mechanical alignment, high reliability, and exact dose delivery. Although clinical results documenting proton radiosurgery to have comparable effectiveness to other modalities have been printed,36-40 randomized trials have by no means been conducted. Introduction to the utilization of protons and heavy ions in radiotherapy: historical perspective. A new stereotactic alignment system for charged-particle radiosurgery on the Harvard Cyclotron Laboratory, Boston. Stereotactic radiosurgery: fundamental ideas, delivery platforms, and medical purposes. Transposition of target data from the magnetic resonance and computed tomography scan pictures to conventional x-ray stereotactic house. Computer-assisted positioning of radiotherapy sufferers utilizing implanted radiopaque fiducials. Isoeffective dose parameters for brain necrosis in relation to proton radiosurgical dosimetry. Comparison of proton and x-ray conformal dose distributions for radiosurgery functions. Relative biological effectiveness of modulated proton beams in varied murine tissues. Gorgulho n Nzhde Agazaryan the idea of focusing external beam radiation to pay attention the dose on the pathology and spare the peripheral constructions appeared in the literature in 1906. During the next years the thought advanced with spiral converging beams, pendulumdirected beams, and eventually, inflexible hemispheric hooked up beams directed with stereotactic precision. As extensively described, Leksell hooked up an x-ray tube to his stereotactic frame and carried out radiosurgery on the primary patient by concentrating on the trigeminal ganglion for the treatment of trigeminal neuralgia. Radiosurgery evolved over the past half of the past century in association with the explosion of imaging strategies. Functional applications were primarily based on the rules of functional neurosurgical localization, an example being visualization of the anterior commissure and posterior commissure on ventriculography to information targeting. Please see the sections "Stereotactic Precision Requirements" and "Production of the Beam" on Expert Consult. However, on account of the move point traits of converging beams, the maximum radiation level is often situated slightly superior to the isocenter when planning intracranial radiosurgery because the a quantity of radiation fields enter from the highest of the top, which brings the "sizzling spot" to a site barely above the isocenter. Leksell and Larsson designed the first gamma unit with 179 cobalt 60 sources and slit collimators to generate an oval-shaped lesion and thereby mimic the warmth lesion made with a radiofrequency probe. The lesion is then completed by growing the temperature past the level wanted to denaturize protein. Notice the sharp dose falloff to keep away from the optic apparatus and the brainstem (arrow). Recurrence of this skull base meningioma was treated with stereotactic radiotherapy. Formation of the lesion after a excessive dose of radiation takes place in a number of phases because of the power of cells to program apoptosis60 and make adjustments in their machinery to supply neurotransmitters29 and hyaline materials. The falloff distance, or the volume of tissue receiving a minimum of 50% of the dose, is proportional to the diameter of the collimator as a outcome of circular collimators are traditionally used for practical radiosurgery. Notice the dose distributions of the 3-mm collimator (B), 4-mm collimator (C), and 5-mm collimator (D). PrescribingtoaVolume Considerations of Volumetric Dosimetry the simplest dose distribution is achieved with a radiosurgery plan involving a single collimator. Such a margin may embody microdissemination of malignant cells surrounding the realm defined by the contrast enhancement. Consideration of the dosimetric consequences of the penumbra is important because the radiation dose could additionally be still sufficiently excessive to cause toxicity in eloquent structures neighboring the lesion, such because the brainstem, motor space, and spinal twine. In these situations, one potential method is to barely underdose the boundary of the lesion touching the eloquent construction in order that the dose falloff happens inside the lesion and not on the border of the lesion or exterior the contrastenhancing limits and extra three-dimensional margins. C, Dose distribution to avoid supply of high isodose volumes to the pontinemesencephalic region. Notice the cold spots (white arrow) and sizzling spots (black arrow) contained in the intensity-modulated radiotherapy target quantity. It is intuitive to grasp that a single collimator will distribute the radiation homogeneously all through that space. To enable steeper dose falloff in that particular border of the lesion, that space is taken into account cold and the beams are organized in such a fashion that many points inside the lesion become hot or chilly to permit eloquent buildings to be spared. Although hardly important, less volume of regular tissue irradiated may account for fewer problems, even when treating massive volumes. With regard to treatment of an acoustic neuroma, for example, the place the facial nerve is operating in the anterior border of the neuroma, a dose of 3. Proper association of optimal isocenter and collimator measurement to realize conformity in complex lesions is an art. Although modern software has automated simulation of the most effective arrangement, time and judgment by the medical physicist and medical group are still required to make the final determination. Furthermore, the flexibility of the delivery system to carry out the prescribed plan with a quantity of isocenters in a reasonable time frame is limited, which might result in a compromise in conformality. Shaped-Beam Techniques Taking advantage of the ingenious thought of the collimator, the multileaf collimator was developed. It is a sensible strategy to avoid undesirable supply of radiation to eloquent structures. The radiation dose is represented on the x-axis and the volumetric share of the structure on the y-axis. The differential format shows histograms during which the peak of every bin reflects the percentage of volume receiving a given dose within that Calc. The y-axis represents the volumetric percentage of the given structure, and the x-axis represents the share of the radiation dose delivered. The double vertical line shows that zero volume of brainstem is receiving one hundred pc of the radiation dose.
Diseases
The / ratio is the one dose at which overall cell killing is equally attributable to each elements of cell killing (D = D2 or D = /) gastritis ulcer prevacid 15 mg order free shipping. Late-responding tissues such because the mind or spinal wire have an / ratio of approximately 2, whereas many tumors have an / ratio of nearly 10 chronic gastritis weight loss 30 mg prevacid free shipping. Noticethatphotonbeamshave a "buildup area" that gives a measure of pores and skin sparing on the surfaceofthepatient gastritis symptoms bupa buy prevacid 30 mg lowest price. Proton beams deposit many of the dose on the endoftheirrange,aphenomenonknownasa"Braggpeak. Free Radicals When cells are irradiated with ionizing radiation, photons can interact with water molecules by stripping an electron from a hydrogen atom, which ends up in a fast electron and an ionized water molecule. The ensuing fast electrons additional interact with water molecules through extra ionizing occasions. The hydroxyl radical is reactive and has sufficient power to interrupt chemical bonds in close by molecules. This indirect impact of radiation via a free radical middleman is accountable for the majority of radiation-induced injury. Tissue hypoxia (Po2 <30 mm Hg) will inhibit the manufacturing of free radicals and thereby lessen the damaging effects of radiation. Double-strand breaks are harder if not unimaginable to restore; they cause the most severe biologic harm. Double-strand breaks could also be the result of a single particle or the interplay of two single-strand breaks attributable to separate particles occurring at shut temporal and spatial distances. There are benefits and disadvantages to fractionated radiation remedy and radiosurgery. Certainly, there seems to be little benefit to fractionation for functional cases. Experimental studies and medical observation have instructed that aerated cells turn out to be nonviable after irradiation and that the site of irradiation is dominated by hypoxic cells. However, proof has demonstrated a phenomenon known as reoxygenation, whereby tumors may reestablish their oxygenated state between sessions if the radiation is delivered in fractions. Through reoxygenation, a higher share of tumor cells shall be depopulated by fractionated irradiation. A number of elements are concerned within the strategy of reoxygenation, similar to decreased oxygen consumption by useless cells and a discount in the variety of cells in relation to capillary blood provide. Malignant tumors usually fall into the category of earlyresponding tissue containing hypoxic cells, whereas normal mind tissue consists primarily of late-responding tissue containing well-aerated cells. Fractionation will increase the mobile depopulation of a tumor for a given total radiation dose because of the phenomenon of reoxygenation. At the identical time, fractionation reduces the injury to crucial late-responding normal tissue. However, fractionation allows malignant tumor cells to repopulate between fractions. The standard approach to radiotherapy consists of every day therapies preceded by a dose supply simulation by which affected person positioning relative to the treatment machine is confirmed to result in applicable beam entrance and exit sites. The use of cross-firing beams permits supply of excessive doses to the region of the target whereas minimizing the dose to surrounding tissue. Although a single radiation beam coming into a affected person begins with a area of excessive dose (after the initial build-up region) and progressively decreases in dose with increased depth, with crossfiring beams the dose at depth progressively will increase as the various beams intersect. Thus, because the dose is deposited alongside each beam, the entire dose absorbed by regular tissue may be stored low while reaching a a lot greater dose at the intersection of the beams and a steep dose gradient between the low- and high-dose areas. This speedy falloff in radiation dose is the basic principle used to spare regular tissue in radiosurgery. Although cross-firing can be used in conventional radiotherapy, its sensible limits are two to 4 fields, and accuracy of supply is on the order of 1 cm or higher in many anatomic websites. However in radiosurgery, as a end result of hundreds of beams are added collectively, the isodose lines start to tackle the configuration of the tumor, thus minimizing dose outdoors the target. He described using radiation as a method of changing the scalpel or electrode for functional neurosurgery. In so doing, the biology of differential restore was discarded, and the principle biologic advantage turned the ability to destroy focally identified areas and avoid normal brain tissue by bodily means. The preliminary radiosurgical idea of Leksell was meant for the treatment of practical neurological issues, however it has now expanded to turn into a regular treatment choice for quite a few benign and malignant central nervous system pathologies. Obliteration of the vascular provide with accompanying endothelial injury of vessels to the tumors additionally appears to play a means more important position in radiosurgery than in radiation remedy. The field of radiation remedy started to grow within the early 1900s, largely due to the groundbreaking work of Nobel Prize�winning scientist Marie Curie, who discovered the radioactive parts polonium and radium. Radium was utilized in various types until the mid-1900s, when cobalt and cesium models got here into use. Lower vitality superficial and orthovoltage x-ray mills were developed and had been helpful in treating shallow targets. In exterior beam radiotherapy, radiation beams travel a distance to the affected person from a radiation source (usually an x-ray, gamma-ray, or electron beam source). Brachytherapy is a method by which a radioactive supply is implanted within the target. Conventional Radiotherapy External beam radiation most commonly makes use of x-rays, gamma rays, or electrons and is the most typical form of therapeutic radiation for cancer treatment. Early external beam items could generate x-rays with only comparatively low power and obtain just a superficial depth of penetration. These machines work by accelerating electrons to excessive kinetic energy and directing them to strike a target with excessive atomic quantity. High-energy electrons interacting with the target materials cause the creation of x-rays primarily by bremsstrahlung interactions. The ensuing x-rays are then formed with collimators and flattening filters to achieve a desired subject dimension and beam traits. At the first Scandinavian neurosurgical assembly held in Oslo, Leksell left the convention room during a lower than thrilling presentation and decided to stroll in a backyard. Leksell confessed to Cairns his doubts in regards to the state of neurosurgical strategies available at the time and was satisfied that one thing new had to be developed. He also mused concerning the thought of utilizing narrow-beam x-rays or ultrasound as the physical agent and removing the probe completely. His enthusiasm and ideas got a warm reception by Cairns, and the inspired younger Leksell began work that led to the development of an "arc-radius" type of stereotactic system. Building on the work of radiation therapists who were treating pituitary adenomas with higher dose, decrease fraction protocols, Leksell postulated that a single fraction of radiation could be much more helpful for intracranial pathology. In the next 10 years, Leksell made appreciable progress in the remedy of deep brain buildings with a single heavy dose of radiation. He collaborated with physicists Kurt Liden and Borje Larsson to make use of a proton beam for radiosurgery. Leksell additionally tried focused beam ultrasound, however this too lacked precision and required that a cranial defect be made earlier than its use. The first stereotactic Gamma Knife unit was put in in Sophiahemmet Hospital in 1968. Leksell wrote that, "Maybe crucial lesson learnt on the Karolinska is that the simplicity of using the Gamma Unit makes this integration potential and that the same individual could be a competent microsurgeon and in addition a stereotactic radiosurgeon. Someone competent in both techniques is greatest fitted to determine the place the boundaries between the 2 methods ought to lie. Innovative work in the area of radiosurgery involving the usage of heavy particles from cyclotrons was also performed by Raymond Kjellberg, Jay Loeffler, and Jacob Fabrikant. Brachytherapy In contrast to exterior beam therapy, in brachytherapy a radioactive supply (or array of sources) is positioned throughout the affected person and left for a predetermined interval. This technique permits excessive local doses of radiation whereas minimizing harm to surrounding tissue, but it can be used just for websites which are accessible via both current physique cavities or surgical insertion. Because brachytherapy offers with radioactive nuclides, security in handling is a concern. Afterloading techniques with machines that automatically load the radioactive sources and using low-energy isotopes have greatly increased radiation security. If considered from the point of view of traditional radiotherapy principle, lack of homogeneity is an intrinsic weak point of brachytherapy for stable tumors.
A randomized, double-blind, controlled trial: intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low again ache gastritis diet in spanish purchase prevacid 15 mg online. Quality of life assessment in sufferers undergoing nucleoplasty-based percutaneous discectomy gastritis and chest pain cheap 30 mg prevacid with visa. Discographic-anatomical correlation of developmental changes with age within the intervertebral disc gastritis symptoms when pregnancy 30 mg prevacid generic mastercard. Predictors of successful consequence for lumbar chemonucleolysis: evaluation of 3000 cases during the past 14 years. Rationale, principles and experimental evaluation of the concept of soppy stabilization. Influence of a dynamic stabilization system on load bearing of a bridged disc: an in vitro research of intradiscal strain. The dynamic neutralization for the backbone: a multi-center examine of a novel non-fusion system. Clinical outcomes of the Dynesys dynamic neutralization system: 1-year preliminary outcomes. Alternative strategies for lumbar discectomy: intradiscal electrothermy and nucleoplasty. The common problems embrace infection, screw misplacement, fusion failure (in the hybrid constructs), persistent pain, and ache on the bone harvest site. Screw-bone interface failure, as recognized by halo formation round a screw, occurred about equally (approximately 5%) in both the semirigid fixation group and the Dynesys group within the U. Should the surgeon deem this discovering to be symptomatic, the surgeon has the choice of revising the system to fusion (in the case of instrumented nonfusion) or revision of the fusion (if the system was used as a fusion adjunct). The magnitude of the stress and the number of cycles over time can moderately be expected to vary from patient to patient, and may be influenced by the sort of nonfusion assemble Full references can be discovered on Expert Consult @ Mummaneni the distinct biomechanical properties of the lumbosacral spine at the aspect of the widened cancellous pedicles distinctive to the sacrum make fusions of this area especially difficult. Certain advanced backbone procedures, corresponding to long phase fusions for scoliosis, place significant biomechanical stresses on the sacral fixation site. Augmentation of a traditional lumbosacral assemble with pelvic fixation should be thought-about under these circumstances. The internal iliac artery and vein, middle sacral artery and vein, sympathetic chain, lumbosacral trunk, and rectum all lie immediately over this construction and stay weak to injury throughout instrumentation of this area. The ilium is demarcated posteriorly by the posterior superior iliac spine, which is an important landmark for iliac instrumentation (see Operative Technique section). The understanding of this anatomy is necessary to realize solid buy for iliac screws. The sacroiliac joint capabilities primarily to transfer axial masses to each hemipelvis and permits virtually no motion. The most rostral aspect of the sacrum has an anterior-posterior diameter of forty five to 50 mm, which tapers to 20 to 30 mm at its most caudal point. Two main issues grew to become evident when attempting to fuse the lumbosacral backbone with this instrumentation. First was the high rate of pseudarthrosis and second was the rate of sacral hook dislodgment. Ferguson and Allen additional modified the Luque system of segmental instrumentation by inserting angled rods into the iliac bones and passing them into hard cortical bone above the sciatic notch to achieve a rigid fixation of the lumbosacro-pelvic backbone. However, the inherent limitations, primarily related to complex threedimensional contouring of the rod before its insertion into the ilium, prompted the development of different methods for lumbosacropelvic fixation. The technical problem of contouring rods for the Luque-Galveston technique was overcome by the introduction of iliac screw instrumentation. They have the additional advantage of modularity, facility of placement, and the capacity to position up to two screws on each side. Furthermore, the biomechanical properties of a threaded screw design, as opposed to the sleek Galveston rod, makes it less inclined to tug out. These flexion forces stress lumbosacral fixation and might lead to screw pull-out and/or pseudarthrosis. The distinct anatomic and biomechanical properties of the sacropelvic area permit for its conceptual division into three zones: zone 1 consists of the proximal sacrum, zone 2 includes the alar wings to the distal sacrum, and zone 3 includes the ilium. Given the broad cancellous pedicles unique to the sacrum, the trajectory of these screws should converge toward the tricortical point of the sacral promontory for optimum fixation. In zone 2, alar screws could also be used to enhance zone 1 instrumentation and thereby improve sacral fixation by as a lot as 20%. Finally, probably the most important biomechanical anchor for sacral fixation is provided by instrumentation of zone 3, the ilium. Iliac screws provide robust resistance to flexion and pull-out forces and are perfect to reinforce L5 and S1 screw fixation. The sacrum Operative Technique for Pelvic Screw Fixation the affected person is positioned susceptible on bolsters that help the chest and anterior pelvis (Table 296-1). A midline incision is made above the level to be fused and extended downward to the underside of S2. Subperiosteal dissection of the lumbar paraspinous muscles is carried out with Bovie cautery and periosteal elevators. We choose to position the hardware cephalad and do any necessary decompression of the neural elements before exposing the midsacrum and posterior superior iliac backbone to limit blood loss from muscle publicity. Subsequently, subperiosteal dissection is extended over the midsacrum and laterally to expose the medial overhang of the ilium. The posterior superior iliac backbone, including the distal overhang of this construction over the sacrum, is uncovered. The entry point for the pelvic screw, which is 1 cm rostral to the palpated inferior overhang of the posterior superior iliac spine and 1 cm beneath the superficial ridge of the posterior superior iliac backbone, is identified. It is necessary to place the screw head deep to the superficial ridge of the posterior superior iliac spine as a result of this structure is the most distinguished bony construction that people feel after they sit in opposition to a tough backed chair. Following the publicity, the pelvic screw entry level is decorticated with a small drill. The pelvic gear shift is then positioned into the entry point and aimed towards the thick bone, which is simply superior to the higher sciatic notch and doubtlessly onward towards the anterior inferior iliac backbone, taking care not to violate the top of the acetabulum. The gearshift is progressively advanced 60 mm or more to achieve the goal bone above the greater sciatic notch. Care have to be taken to not enter the greater sciatic notch itself to keep away from injuring the neurovascular buildings that traverse it. Anteroposterior fluoroscopy sometimes offers enough steering to direct the pelvic gear shift to the bone just superior to the higher sciatic notch. The angle of the gear shift from the entry point is usually 30 to forty five degrees inferiorly within the coronal plane and 30 to forty five degrees anteriorly in the axial airplane. A frequent problem encountered throughout advancement of the pelvic gear shift is to violate the superficial cortex of the ilium before reaching the goal bone above the greater sciatic notch. This typically occurs as a outcome of the pelvic gear shift is directed too superficially within the axial plane. Another potential pitfall is entry of a part of the probe into the sacroiliac joint with subsequent violation of the anterior cortical wall of the pelvis. Early in our expertise, we dissected the gluteal musculature off the dorsal floor of the ilium lateral to the posterior superior iliac spine so as to palpate the "downslope" of the ilium to guide our axial angle. Specifically, pelvic inlet views and obturator views might help to information the pelvic screw down the intended trajectory. We then faucet the hole with an undersized faucet (typically 6 mm in width) and then place the pelvic screw (typically 7 to eight mm in width and sixty five to 80 mm or more in length). We take care to avoid violating the sacroiliac joint with this and subsequent steps. Subsequently, the pelvic screw is then threaded into the pilot hole until the head of the screw is recessed into the posterior superior iliac backbone. This step in screw placement is important as a outcome of recession of the screw head into the bone prevents the patient from feeling a prominent screw head when he or she sits against a hard-backed chair. However, burying the screw heads below the superficial portion of the posterior superior iliac spine helps to stop superficial skin breakdown and pressure sores in these sufferers. It is necessary to create the pelvic screw connection to the lumbosacral rod inferior to S1 to keep away from interference of rod linkage with the S1 screw (if present). Thus the affected person underwent a long segment correction and fusion of her kyphoscoliosis. Given the massive flexion forces that may outcome from the length of this construct, the decision was made to increase the instrumentation to the pelvis. The patient underwent T3-S1 pedicle screws with bilateral pelvic screws followed by L4-5 and L5-S1 anterior interbody fusion.
Laws and colleagues analyzed 86 sufferers handled by microsurgery alone and reported biochemical remission rates of 87% and 51% for microadenomas and macroadenomas, respectively gastritis gerd symptoms purchase prevacid 15 mg mastercard. The largest surgical sequence, by Nomikos and associates in 2005, reported on 688 sufferers, 506 of whom underwent primary transsphenoidal surgery for their acromegaly gastritis yeast infection purchase 30 mg prevacid with mastercard. Again, sufferers with microadenomas had higher biochemical remission rates than did these with macroadenomas (75% versus 50%, respectively) gastritis diet 5 bites 30 mg prevacid cheap mastercard. It ought to be cautioned that an enormous vary of success rates have been reported within the revealed literature, principally because of diversified definitions of biochemical management or treatment. The surgical morbidity in experienced arms is kind of low: reported mortality rates are lower than zero. These outcomes reveal that biochemical management increases with time after remedy. In one other massive research, Barrande and coworkers monitored 128 patients for a mean interval of eleven. Because of their nonsecretory nature, these tumors commonly have an effect on anterior visible structures such as the chiasm and cause visual field defects or have an impact on visual acuity (or both). In one other examine, Turner and associates analyzed the end result data of seventy three patients handled by surgical procedure only and observed for a mean of 6. In a 2006 study, Dekkers and coworkers found solely a 10% recurrence price in 97 sufferers handled surgically at a mean follow-up time of 6 years. Surgical administration of vestibular schwannoma and radiosurgery of benign tumors are thought of separately in Chapters a hundred thirty and 256, respectively. Tumor control is the principal purpose of the administration of these tumors, but because of the benign nature of most of those tumors, long follow-up durations are required to determine this outcome. Conservative administration of these tumors relies completely on their protracted pure history. Studies of sufferers managed conservatively reveal wide-ranging progress rates (between 0 and 30 mm/yr), however with a median growth price ranging from zero. Conservatively managed patients- and possibly even those who bear nonsurgical management- require lifelong follow-up. Facial nerve preservation is an important goal within the administration of vestibular schwannomas. Facial paresis is disfiguring and associated with important social and psychological trauma. Hence, control of tumor growth, by whatever therapy methodology, has the potential to protect facial operate. Hearing preservation grew to become such a discriminator and is a further metric that defines successful treatment. However, evaluation of which technique is one of the best in preserving listening to has been mired in controversy relating to what constitutes good or acceptable hearing. Frequently, patients in whom small vestibular schwannomas are diagnosed but who retain helpful listening to have been managed conservatively on the assumption that hearing might be preserved if the tumor stays static. The converse can additionally be true, with well-described listening to loss in patients with radiographically secure tumors. These charges fall dramatically with increasing tumor measurement,164,171 but general, a hearing preservation price of 50% or greater could be anticipated with small tumors (<2 cm). It can be value noting that listening to preservation is frequently glorious within the early postoperative interval however that delayed hearing loss unrelated to tumor recurrence has been reported increasingly with extended follow-up. Most studies have reported very high rates of listening to preservation, 53% to 98% (see Table 251-5). The most typical of those neuropathies includes the trigeminal nerve and, less frequently, the glossopharyngeal/vagal nerve advanced. The trigeminal complicated gives rise to signs in about 10% of sufferers as part of the natural history of the tumor, and the extent as well as the severity of signs is largely a perform of tumor dimension. Hydrocephalus was completely absent in a single reported collection,146 whereas it was reported in 11% of patients in one other. This is basically because of the glorious tumor management and toxicity profile, which, it might be argued, is superior to either surgery or single-fraction radiosurgery. Surgery is one of the best preliminary treatment possibility but may be restricted in the area of the cranium base or hypothalamus, the place its proximity to crucial constructions precludes full resection with acceptable morbidity. Aggressive surgery is more likely to achieve complete tumor elimination but regularly at the worth of excessive therapy mortality and morbidity. In one of many older studies, Regine and associates demonstrated a 44% threat for relapse with doses of lower than 54 Gy as in contrast with simply 16% at larger doses,209 however only a small number of patients were used to derive this dosimetric threshold. Similarly, Habrand and coauthors reported that better tumor control was achieved with a dose of fifty five Gy or higher than with lesser doses. For these reasons, weekly or biweekly imaging throughout therapy is advisable to make certain that the enlarged cyst remains within the handled volume. The risk for optic nerve injury is related to the total dose and fraction measurement as described earlier within the section "Meningioma"; optic nerve harm is quite uncommon with a total dose of up to fifty four Gy delivered in 30 fractions. These remedies permit the use of smaller therapy margins and consequently reduce the dose to regular brain tissue. The most common late complication of treatment is hypopituitarism, with neurocognitive impairment, optic neuropathy, and radiation necrosis being less frequently reported. Recurrences could also be noticed several years after therapy, and patients incessantly survive for a quantity of years after recurrence has been detected. For example, Fagundes and associates reported on 204 sufferers with chordomas arising in the base of the skull or the cervical backbone who had been treated between 1975 and 1993; sixty three patients (31%) experienced recurrence. The majority (73%) of the recurrences have been native; 2 patients (3%) experienced nodal failures, three patients (5%) had seeding of the surgical observe, and distant metastases developed in thirteen sufferers (21%). Gay and coauthors reported on forty six patients with cranium base chordoma and 14 sufferers with chondrosarcoma who underwent surgical procedure between 1984 and 1993 at the University of Pittsburgh, 50% of whom had a history of previous treatment. Maira and colleagues reported on 12 sufferers with clival chordomas who have been treated surgically and monitored for a mean period of forty months (range, 14 to 86 months). Similarly, Thieblemont and associates reported on 8 sufferers with cranium base chordomas treated surgically. Four patients had been alive with illness at 40 to 59 months of follow-up, 2 patients died with tumor at 13 and fifty three months, 1 affected person was alive and illness free at 2 months, and 1 affected person was alive at one hundred thirty months (disease standing not reported/ unknown). For example, Al-Mefty and Borba reported one postoperative death and permanent neurological deficits in two patients, together with visible subject defects and oculomotor nerve palsy, among those that underwent surgery for cranium base chordoma. Altogether, 9 of 13 sufferers (69%) died with locally recurrent tumor, 1 patient was alive with recurrent tumor at 49 months, 2 sufferers (15%) have been alive and disease free at 10 and one hundred forty four months, and 1 patient was lost to follow-up. The reported local management charges at 5 and 10 years had been 59% and 44%, respectively. Interestingly, the authors noticed that decrease local control rates were related to feminine gender, lower minimal tumor dose, and higher inhomogeneity. Several authors have confirmed the affiliation between reduced native management and feminine sex and posited hypotheses for such observations. Noel and coauthors reported the following issues after therapy of sixty five patients with skull base chordomas or chondrosarcomas: hypopituitarism (25%), memory impairment (2%), oculomotor impairment (3%), profound hearing loss (2%), and bilateral visual loss (2%). In the present era, advances in remedy planning and supply of high-dose, hypofractionated treatments (5 Gy/fraction) are prone to be increasingly explored for the therapy of these tough cranium base tumors based on the assumption that hypofractionated remedies are extra likely to overcome the perceived radioresistance of these tumors. Despite being a separate pathologic entity from skull base chordoma, both tumors are sometimes described together and managed equally because of their rarity and scientific findings. Chondrosarcomas are believed to come up from the cartilaginous matrix of the skull base (or from primitive mesenchymal cells) near the petroclival junction or different fused junctions. For example, Korten and coauthors reported a local recurrence rate of 53% in sufferers treated by surgical procedure alone. It is due to this fact advisable to manage cranium base chondrosarcomas in a way analogous to that of chordomas. Stereotactic radiosurgery and fractionated stereotactic radiotherapy for the remedy of acoustic schwannomas: comparative observations of one hundred twenty five patients handled at one establishment. Short- and long-term issues of radiation remedy for pediatric brain tumors. Prognostic elements and results of radiotherapy alone within the management of pituitary adenomas.
Although extra radical decompression is often necessary to adequately relieve neural compression, some studies have determined that limited resection of the articular course of with or with out in situ intertransverse fusion has significantly better results than aggressive facet joint resection with out fusion and that decompression without fusion has good outcomes with solely limited development of slippage, supplied that pars and side joint integrity is preserved gastritis shortness of breath prevacid 30 mg cheap mastercard. Kornblum and coworkers associated pseudoarthrosis with worse medical outcomes in a long-term outcomes research of patients treated with decompression, decompression and bone fusion, and decompression and instrumented fusion gastritis diet milk prevacid 15 mg buy without prescription. It offers a method of correcting the slip angle and may be performed with or with out reduction xenadrine gastritis prevacid 15 mg with amex. Improved fusion charges for higher grade spondylolisthesis65 and extra aggressive decompression could be achieved through instrumentation. Although each groups demonstrated vital improvement, blood loss and longer operative instances had been famous in the instrumented group. Other studies have demonstrated realignment alone with out decompression to be adequate for achieving good outcomes (satisfactory aid of again pain in 89% and improvement in radicular symptoms in 93%) in sufferers with unstable slippage. Better restoration of sagittal steadiness and discount of slippage were proposed as elements in the enchancment in again pain with instrumentation. Despite a high fee of fusion in each groups, of their examine of greater than 40 sufferers undergoing posterolateral fusion without decompression for isthmic spondylolisthesis, Haraldsson and Willner discovered important aid of symptoms in 95% of adolescents, whereas only 57% of adults reported the same diploma of enchancment. The use of interbody grafts for the remedy of spondylolisthesis is a common strategy. Together with posterior instrumentation, interbody grafts have demonstrated superior stability in cadaver research compared with standalone anterior cages or posterior-only instrumentation for degenerative spondylolisthesis. Both anterior lumbar interbody fusion and posterolateral fusion were mixed with pedicle screw fixation to augment the fusion in this research. However, there are inherent complications that must be thought-about when proposing an anterior method, and the results are various in comparison to posterior approaches. Nonoperative measures should be the first-line treatment, with surgical intervention being reserved for patients who clearly fail conservative algorithms. The proposed surgical procedure ought to be tailor-made to each patient and is dependent on elements such as patient age, the presence of a neurological deficit, and the kind of spondylolisthesis. The goal of therapy is to supply a long-term steady assemble that provides enough decompression to allow the patient to return to and maintain a normal state of functioning. Future directions will concentrate on each conservative therapy strategies and enhancements in surgical technique. Prospective randomized scientific research, the event of new technology, and translational research will drive the development of latest treatments to offer our sufferers affected by this situation. Surgical therapy of spondylolisthesis without spine fusion; excision of the unfastened lamina with decompression of the nerve roots. Classification of high-grade spondylolistheses based on pelvic version and backbone stability: potential rationale for discount. Lumbar sagittal stability influences the medical consequence after decompression and posterolateral spinal fusion for degenerative lumbar spondylolisthesis. Results of degenerative spondylolisthesis handled with posterior decompression alone through a model new surgical strategy. Direct repair of the pars interarticularis for spondylolysis and spondylolisthesis. A proposal for a surgical classification of pediatric lumbosacral spondylolisthesis based mostly on current literature. Nonsurgically managed sufferers with degenerative spondylolisthesis: a 10- to 18-year follow-up study. Spondylolisthesis in youngsters and adolescents: surgical remedy with and without dorsal transpedicular instrumentation. Surgical therapy of severe isthmic spondylolisthesis in adolescents: discount or fusion in situ. Long-term medical and radiological follow-up of spondylolysis and spondylolisthesis. Ames Adult scoliosis is defined as any lateral curvature of the backbone in a skeletally mature particular person with a Cobb angle of larger than 10 degrees in the coronal aircraft, the lumbar and thoracolumbar levels most often being affected. Diskography, side blocks, and epidural steroid injections may be used as ancillary tests to further correlate the clinical symptoms with radiographic abnormalities. The choice to provoke treatment is primarily based on proof of continued curve progression and unrelieved ache. Cosmetic considerations are much less typically an indication for remedy within the common adult population, although they could turn into more necessary to young adults. The targets of surgical treatment are each elimination of symptoms and restoration of spinal stability. Surgical treatment of adult scoliosis has evolved tremendously within the previous 30 years, largely as a result of developments in spinal instrumentation by Harrington, Dwyer, Luque, Zielke, CotrelDubousset, and their colleagues. This chapter discusses the analysis, management, and medical outcomes of sufferers with grownup scoliosis with an emphasis on involvement of the thoracolumbar backbone. In common, de novo scoliotic curves have less of a coronal airplane component than sort 2, or progressive idiopathic scoliosis. Because de novo scoliosis is primarily the results of a degenerative course of, spinal stenosis from disk degeneration and side hypertrophy is extra frequent in these patients than in these with progressive idiopathic scoliosis. Musculoskeletal back pain can be localized on the apex of the curve or at its concavity, and the areas above and below the curve may be painful from excessive stress on the side joints. This sort of musculoskeletal ache is a results of each excessive strain and fatigue on the paravertebral muscles as they try and compensate for the loss of regular spinal steadiness, as well on account of true spinal instability inflicting abnormal stress on the side joints. Radicular ache may also be attributable to traction of nerve roots on the convexity of the curve. Intercostal neuralgia secondary to rib cage deformity can be seen in sufferers with extreme thoracic and thoracolumbar curves. In the latter state of affairs, the back and radicular ache is usually relieved when recumbent because the spine, disks, facet joints, and neural foramina are unloaded. The visible analogue scale should be used to quantify the severity of ache and is effective in reporting changes in ache after treatment. Type 1 contains scoliosis secondary to iatrogenic causes, vertebral fractures, degenerative adjustments, and osteoporotic disease. Bowel or bladder dysfunction might sometimes occur on account of compression of the cauda equina. Curve Progression Progression of scoliotic curves may be manifested as modifications in clothing measurement or peak or frank alterations in body shape, such as a rib hump. Progression occurs in both grownup degenerative and adult idiopathic scoliosis, though it has been found to happen more quickly within the latter group. Cosmesis Unlike the situation within the adolescent inhabitants, cosmesis is a relatively infrequent criticism by grownup scoliosis patients. Patients younger than 40 years, nonetheless, may often have a chief criticism of an unacceptable cosmetic deformity from progressive idiopathic scoliosis. A historical past of idiopathic scoliosis should be documented, in addition to symptoms of curve progression. Medical comorbid circumstances such as osteoporosis, diabetes, obesity, and poor diet are documented and addressed throughout a radical history. The bodily examination ought to start with a general inspection of the affected person within the standing place with knees and hips absolutely extended. The location and severity of spinal curves, rib humps, sagittal and coronal stability, pelvic obliquity, curve flexibility, and any leg size discrepancies must be famous. Moreover, an evaluation of hip flexibility must be performed to rule out a hip contracture as the cause of the sagittal imbalance. Improvement in posture after sitting usually indicates a hip flexion contracture. The affected person must also be examined within the supine position for evidence of improvement in sagittal and coronal alignment. A rigid thoracic kyphosis is usually indicated by the persistence of a kyphotic deformity in the supine position. A thorough neurological examination is performed to evaluate for abnormalities resulting from compression of nerve roots or the twine (or both). Gait and reflexes ought to be evaluated for proof of myelopathy from thoracic canal stenosis.
Flaggon (Orris). Prevacid.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96636
In a evaluation of 62 patients treated at 71 sites, 27 (38%) had progressive, vertebral physique fractures, only 7 (11%) of which have been associated with illness development gastritis diet what to eat for breakfast lunch and dinner generic prevacid 15 mg free shipping. Additionally, sufferers with 40% to 80% lytic destruction of the vertebral physique had an 85% (11/13) chance of progressive fracture gastritis cure home remedies order prevacid 15 mg free shipping. Bisphosphonate therapy could scale back the danger for fracture, although the mechanism of fracture might be osteoblast inhibition or cell death rather than osteoclast activation gastritis symptoms in cats 15 mg prevacid order. Significant patient advantages embrace shorter treatment occasions and fewer delicate tissue toxicity. Benign spinal tumors represent a gaggle of intradural extramedullary neoplasms that embody meningiomas, schwannomas, and neurofibromas. The major remedy choice for many benign spinal neoplasms is microsurgical resection. In addition, tumors which have recurred after open surgical resection may make protected surgical resection challenging or impossible. It is in such clinical circumstances that radiosurgery might be an essential medical option for these patients. Stereotactic radiosurgery for the remedy of all kinds of benign intracranial lesions has turn into widely accepted and has glorious long-term outcomes and minimal toxicity. In addition, benign backbone tumors have their very own unique scientific manifestations, relationship to the spinal twine, and radiobiologic response to radiosurgery, any of which could characterize distinctive challenges to secure and effective software of radiosurgical ablation. Relative contraindications to spinal radiosurgery embrace evidence of overt spinal instability, neurological deficit ensuing from bony compression, or previous radiation remedy to the spinal twine tolerance dose. A theoretical advantage of using spinal radiosurgery as frontline administration of spinal tumors is the chance that such therapy could act as prophylaxis towards future spinal instability or compression of neural components and thus obviate the need for in depth spinal surgery and instrumentation. Moreover, early radiosurgery might obviate the necessity for large-field external beam radiation, which is understood to suppress bone marrow perform. Tumor shrinkage and full obliteration aside, the minimally invasive technique of spinal radiosurgery might turn into an effective palliative strategy solely via native tumor control. Finally, the flexibility to perform spinal radiosurgery in the outpatient setting is a bonus which will spare patients with spinal tumors each time and the morbidity of hospitalization. The low radiation tolerance of the spinal wire is the first limiting factor within the dose of therapeutic ionizing radiation that can be used for spinal tumors. Conventional exterior beam radiotherapy lacks the precision to deliver large single-fraction doses to benign spinal tumors in shut proximity to the spinal cord. In fact, the radiosensitivity of the spinal cord has usually required that the therapy dose be far beneath the optimal therapeutic dose. The intradural nature of benign spinal tumors engenders a close proximity between the tumor and spinal wire or cauda equina, an anatomic relationship that will influence the chance for neural toxicity. Moreover, as a outcome of benign spinal tumors are prone to late recurrence and the late toxicity of radiation delivered to the spinal cord may take years to develop, analysis of radiosurgical treatment when it comes to efficacy, safety, and sturdiness will necessitate longer follow-up than what has been granted to patients with metastatic spine tumors. Such fusion may improve the goal definition for spinal tumors, particularly when the neoplasms exhibit heterogeneous distinction enhancement. The massive and sometimes irregular shape of spinal neoplasms could make contouring a challenge. Although benign intradural, extramedullary tumors of the spine are sometimes conspicuous by their homogeneous distinction enhancement, the large and often irregular shape of spinal neoplasms makes contouring a serious challenge. The goal of spinal radiosurgery for benign spinal tumors is to deliver a clinically important radiation dose to the tumor via a plan that respects the radiation dose tolerance limits of the nearby spinal cord, cauda equina, and surrounding organs such as the intestines, esophagus, kidneys, larynx, and liver. By virtue of their origin along the dura and spinal nerve roots, extramedullary spinal tumors can considerably impinge on the spinal twine or cauda equina and thus make contouring difficult. The singlefraction doses prescribed for spinal radiosurgery have various from 12 to twenty Gy (Table 263-1). The linear quadratic equation remains the most accepted mathematical model of cell kill secondary to ionizing radiation. The spinal wire is among the most radiosensitive structures thought of in radiosurgical therapy plans. Radiation-induced myelopathy may happen in delayed trend, and the spinal wire tolerance of single-fraction radiation has not been fastidiously decided with long-term follow-up research. Nevertheless, some knowledge level to less than a 5% likelihood of myelopathy at 5 years when the twine receives a 60-Gy dose through standard fractionation. In distinction to patients with metastatic most cancers, patients undergoing radiosurgery for benign paraspinal neoplasms are anticipated to survive longer with greater useful status. Whether previous radiosurgery will sensitize the spinal cord and cauda equina to degenerative insults in aging sufferers is also unknown. Spinal radiosurgery will most likely with time be explored because the initial treatment of each malignant and benign spinal tumors. Given their pathologic similarities, it has been speculated that benign spinal lesions can be equally aware of radiosurgery as their intracranial counterparts. The extramedullary intradural spinal neoplasms handled with radiosurgery have primarily included meningiomas, schwannomas, and neurofibromas. However, the first reported benign spinal tumor treated with radiosurgery was truly a hemangioblastoma. Dodd and associates, within the largest revealed sequence to date for benign intradural extramedullary spinal tumors, reported the results of radiosurgical treatment of 55 such tumors (30 schwannomas, 9 neurofibromas, and sixteen meningiomas). Less than 1 12 months after radiosurgery, three sufferers (one with meningioma, one with schwannoma, and one with neurofibroma) required open surgical resection of their tumor because of persistent or worsening signs. From Gibbs I, Chang S, Dodd R, et al: Radiosurgery for benign extramedullary tumors of the spine. A and B, Gadoliniumenhanced sagittal and axial magnetic resonance imaging demonstrates the tumor filling the spinal canal. C and D, Sagittal and axial projections of the isodose lines of the treatment plan. The tumor was treated with a prescribed dose of 13 Gy in a single fraction to a volume of 3. E and F, Sagittal and axial projections of the cone beam computed tomographic imaging used for patient setup and image-guided radiosurgery. All lesions on this group have been both secure (61%) or smaller (39%), with no tumor rising in dimension. The following sections, subdivided by histopathology, summarize the available scientific end result knowledge for benign spinal tumor radiosurgery. Meningiomas Spinal meningiomas are arachnoid cap cell�derived tumors that develop in people within the fifth to seventh decade, have a female preponderance, and happen mainly within the thoracic area. They arise from cells of the meningeal coverings of the central nervous system and happen extra incessantly within the mind than the spine at a 5: 1 ratio. Only 1 patient required open surgery, and another sustained the one complication reported within the collection. Seventy % of the meningiomas handled on this sequence were symptomatically steady or improved. Eleven of thirteen sufferers underwent radiosurgery as an adjunctive therapy of residual or recurrent tumor after open surgical resection. Radiographic tumor management was demonstrated in all cases with a median follow-up of 17 months. Schwannoma is the most typical spinal tumor and has no proclivity for a particular spinal area or gender. After a imply follow-up of 20 months, half of the patients reported an improvement in signs after radiosurgery, and half reported worsening of pain, weak point, or numbness at their last follow-up. They additional acknowledged that probably the most sensible and attainable aim of remedy of neurofibroma in myelopathic sufferers is tumor control with out vital expectations for improvement in signs. Similar to the Stanford expertise, no patient has had evidence of radiographic tumor progression on follow-up. Furthermore, on situation that lots of the sufferers with neurofibromas have a quantity of lesions alongside their spine, it could possibly often be troublesome to determine whether or not symptom progression is because of the treated lesion or any of the opposite neurofibroma lesions within the spine. A and B, Sagittal and axial projections of the isodose lines of the remedy plan. The tumor was treated with a prescribed dose of 14 Gy in a single fraction to a quantity of 9. Given their posterior position relative to the spinal cord or cauda equina, removing via a laminectomy strategy is usually straightforward.
Biomechanical comparability of two-level cervical locking posterior screw/rod and hook/rod strategies gastritis unspecified icd 9 code safe 15 mg prevacid. Kaiser Reconstruction of the anterior thoracic backbone has dramatically modified prior to now a quantity of a long time gastritis zwieback generic prevacid 15 mg on-line. The early efforts of surgical pioneers to stabilize the spine after destruction of the anterior spinal components were typically met with excessive charges of morbidity and assemble failure gastritis emedicine prevacid 30 mg discount with visa. The evolution of anterior thoracic instrumentation has led to a simplification of insertion techniques, improved biomechanical and imaging characteristics of current implants, and a big reduction within the dangers previously related to anterior thoracic stabilization. This chapter describes the background and surgical practice of anterior instrumentation of the thoracic spine. In the Seventies, advances in assemble design have been launched by Dwyer,4,5 Zielke,6 and colleagues. The screwcable assemble of Dwyer and the screw-rod construct of Zielke successfully corrected scoliotic deformities. In the late Nineteen Seventies, Dunn developed a double-rod, double-screw assemble that supplied sufficient stability for anterior thoracolumbar reconstruction. Less optimum outcomes with an elevated incidence of postoperative issues have traditionally been related to posterior decompression for anterior metastatic illness. An anterior strategy supplies a direct technique of addressing ventral pathology and reconstructing the spine at the major site of instability. Important considerations for applicable affected person selection embrace age, preoperative functional status, presence of medical comorbid circumstances, life expectancy, and want for tissue prognosis. The worth of restoring neurological function, such as ambulation or sphincter control, should be judged on a person basis. Other considerations in choosing sufferers for operative intervention embody the kind of tumor, compromise of the spinal canal, extent of neurological deficits, level of ache, and diploma of instability. Adjuvant remedy similar to radiotherapy, chemotherapy, or hormonal therapy could additionally be indicated in particular cases. Additionally, nonoperative intervention stays an option for sufferers with steady myelopathy despite spinal twine compression. Neurological deterioration is uncommon after operative intervention for metastatic spinal disease. Perioperative mortality charges vary from 6% to 8%, and total complication charges vary from 8% to 11%. Spinal neoplasms can be manifested as ache, progressive deformity, or neurological deficits. Operative intervention is appropriate for tissue prognosis, neurological decompression, and spinal stabilization. Posterior fusion and fixation could additionally be acceptable within the absence of a ventral deformity or anterior spinal canal compromise. Lesions producing ventral compression or important biomechanical compromise of the anterior and middle columns are indications for an anterior strategy. Previous reviews have documented higher outcomes with an anterior method than with isolated posterior stabilization. Loss of the posterior pressure band may require supplementation with a posterior stabilization construct. Patients with a whole spinal wire damage may still profit from spinal stabilization. In such circumstances, surgical stabilization optimizes the rehabilitation course of and possibly decreases the length of hospitalization. Exposure of the higher thoracic spine is difficult by the advanced anatomy of the superior mediastinum, presence of the good vessels, depth of publicity, and kyphotic angulation of the backbone. A midline sternotomy can be utilized however often necessitates the help of a thoracic surgeon. Pathology affecting the middle to decrease thoracic backbone (T5-10) may be accessed with either a posterolateral (lateral extracavitary) or anterolateral (retropleural thoracotomy) approach. For the thoracolumbar area (T10-L2), a thoracoabdominal method during which one of the approaches for the lower thoracic backbone is mixed with a retroperitoneal method offers glorious entry. A more intensive sternal-splitting strategy is usually necessary for anterior entry to the lower vertebrae, sometimes up to the fourth or fifth thoracic vertebrae, or for patients with brief stout necks. These exposures must be performed with the help of an experienced thoracic surgeon and are past the scope of this textual content. It is ideally suited for lesions with a big anterior paraspinal extension, with or without a substantial intraspinal component. This method offers a well-known exposure and orientation for neurosurgeons and in depth entry to all three spinal compartments. In addition, circumferential stabilization of the spine is possible through a single incision. The lateral extracavitary strategy is versatile and can be modified based on the size of the tumor, degree of involvement, relationship to neural buildings, and need for spinal stabilization. Once anesthesia is induced, the affected person is positioned in a threequarter or full susceptible position. Rotating operative tables enable the affected person to be turned through the procedure to gain elevated visualization of the ventral spinal compartment. A number of incisions can provide access via the lateral extracavitary approach, including midline, hockey stick, semicircular, and paramedian incisions. If a "hockey stick" kind of incision is used, adequate caudal publicity is needed before the incision is prolonged laterally, or the caudal extent of the publicity might be limited. Routine subperiosteal dissection of the paraspinal muscles is carried out with a Cobb dissector and monopolar cauterization. The takedown is carried out bilaterally if posterior exposure is required for laminectomy or instrumentation; in any other case, unilateral exposure is sufficient. The lateral limb of the "hockey stick" incision is opened by transecting the transversely oriented thoracic muscular tissues. The myocutaneous flap is elevated to expose the longitudinally oriented erector spinae musculature. An extended midline incision can present comparable access with much less musculoligamentous harm and probably an improved beauty result. Once the transversely oriented muscles are retracted, the lateral margin of the erector spinae is recognized and dissected medially to expose the underlying ribs. Surgery is often reserved for kyphosis larger than 30 degrees, in addition to radiographic proof of progression of the deformity. Clinical indications for operative intervention include intractable axial or radicular ache and progressive neurological deficits. At the thoracolumbar junction, instrumentation is important to resist the dynamic biomechanical forces encountered at this level. Most of those uncommon lesions could be resected successfully by way of a posterolateral method without the addition of fusion and fixation. Mobilization of the erector spinae muscle permits entry to the lateral spinal compartment. The longitudinal muscle mass is wrapped in a moist sponge to keep away from desiccation and positioned medially or laterally to allow the surgeon to work on either facet. Complete dissection of the vertebral elements above and beneath the pathologic degree ensures adequate ventral publicity. The dorsal and lateral rib surfaces are exposed with a Cobb elevator as much as the articulation of the vertebral physique. The ventral gentle tissue is dissected free in subperiosteal style with a Doyen rib dissector. The exposed transverse process on the stage of the pathology, along with 6 to 8 cm of the corresponding rib, is then resected with a rib cutter and rongeur. The costotransverse and costovertebral joints are disarticulated and transected sharply. Resection of the rib head exposes the anterolateral floor of the spine, together with the pedicle and intervertebral foramen. Resection of 3 to four cm of the adjacent ribs can enhance ventral exposure; however, extreme rib resection can lead to a flail chest deformity. Once the rib and transverse processes are eliminated, the neurovascular bundle is recognized throughout the endothoracic fascia, deep to the intercostal musculature.
The muscle layers are reapproximated individually and sewn with a heavy absorbable suture gastritis symptoms hemorrhage prevacid 30 mg purchase with mastercard. Use of an external orthosis such as a thoracolumbar spinal orthosis postoperatively is decided primarily based on the security of fixation and surgeon preference gastritis diet 4 you prevacid 30 mg discount online. Additionally, the placement of anterior instrumentation (vertebral body screws and rods) could also be difficult gastritis symptoms dizziness purchase prevacid 15 mg visa. ParamedianRetroperitoneal Approach(L3-S1) Direct anterior publicity of the distal lumbar ranges may be obtained through a paramedian retroperitoneal route. Compared to the flank method, the paramedian approach provides a more direct anterior publicity and minimizes disruption of the muscles of the anterolateral stomach wall. The paramedian strategy is especially useful for interbody grafting for arthrodesis and for decompression of the spinal canal when bilateral publicity of the vertebrae is important. It can be used for exposure of L5-S1 the place a flank strategy is usually prohibited by the ilium. The patient is positioned supine with a bolster placed beneath the lower back to elevate the sacrum and facilitate the publicity. A vertical (midline or paramedian) or transverse (Pfannensteil) incision may be used, but a paramedian incision offers the benefits of preserving the rectus sheath and allowing rostral or caudal extension if essential. The muscle tissue are retracted to reveal the posterior rectus sheath and transversalis fascia. The transversalis fascia is incised to expose the underlying retroperitoneal fats and the peritoneum. The airplane between the transversalis fascia and peritoneum is developed with blunt dissection, and the parietal peritoneum is free of the lateral stomach wall. The stomach contents and peritoneum, along with the kidney and ureter, are reflected medially to expose the ventral lumbar spine. Dissecting the peritoneum off the ventral belly wall permits full mobilization of the peritoneal contents. The remainder of the dissection is just like the ventrolateral retroperitoneal strategy. TranspsoasApproach(L1-5) In latest years the sphere of minimally invasive surgical procedure has expanded to contain surgical approaches to the spine as surgeons and patients seek novel methods to reduce tissue trauma during surgical procedure, lessen postoperative discomfort, and shorten hospital stays. To this end, a novel approach by way of the psoas muscle provides a lateral method which may be achieved via one or two small (3- to 4-cm) incisions using tubular retractors and avoids the necessity for both a transperitoneal or retroperitoneal anterior method. A second mark is made posteriorly on the border between the erector spinae and abdominal oblique muscular tissues. Blunt dissection is used to unfold the muscle fibers until the retroperitoneal area is reached. The index finger is then used to sweep the peritoneum anteriorly whereas palpating right down to the psoas muscle. Alternatively, a single, barely larger incision could also be made within the flank by way of the muscle layers and blunt retroperitoneal dissection used to dissect medially to the psoas muscle. The dissection happens between the middle and anterior third of the psoas muscle to keep away from the lumbar plexus, which lies dorsally. Sequentially bigger dilators are introduced through the psoas muscle to the annulus of the disk, adopted by the retractor blades. If no response is obtained with careful stimulation, the muscle could then be divided and, if necessary, removed within the confines of the retractor. When the floor of the disk is exposed, the position of the retractor is reconfirmed by fluoroscopy. Further retraction, if essential, must be directed anteriorly to forestall extra strain on the posterior portion of the psoas and the neural elements inside it. On closure the retractor blades are removed slowly whereas hemostasis is carefully confirmed, and the 2 small incisions closed in the usual trend. The distal limit of the transpsoas approach is decided by the peak of the iliac crest. Access to more than two adjacent intervertebral disks requires further incisions. The superior hypogastric plexus is the terminal extension of the preaortic sympathetic plexus. This nice, thin assortment of nerves is mostly discovered arching over the left iliac artery crossing the L5-S1 disk house. The superior hypogastric plexus provides innervation to the inner vesicle sphincter; damage to those nerves can end result in retrograde ejaculation. Great care should due to this fact be taken in clearing prevertebral tissue from the ventral L5-S1 disk area. The use of electrocautery superficial to the anterior longitudinal ligament is prevented. All prevertebral tissues, including the hypogastric plexus, are bluntly swept to the right. The center sacral artery and vein are recognized inferior to the aortic bifurcation and are ligated and divided. L4-5 is best approached laterally to the vessels as a outcome of the origin of the vena cava and the bifurcation of the aorta are usually ventral to L5. If the origins of the vena cava and aortic bifurcation are abnormally high, an interiliac approach may be attempted. The iliolumbar vein must even be recognized, ligated, and divided throughout publicity of L4-5 to permit medial retraction of the iliac vein and access to the disk area. Once the process is accomplished, the belly contents are returned to their regular anatomic position, and the fascial and muscular layers are closed separately. When the spinal process is accomplished, the posterior peritoneum is closed with absorbable suture. The abdominal contents are then returned to their anatomic place to forestall intestinal torsion and obstruction. The particular person fascial and muscular layers are reapproximated with absorbable sutures. This factor resists the compressive forces created by axial loading of the lumbar backbone. Their effect on lateral flexion is variable and depends on the dimensions and shape of their interfaces with the vertebral end plates. To obtain higher rigidity of the overall assemble, fixation of the vertebral bodies is usually carried out. This may be either with anterior vertebral fixation with a screw rod or plate instrumentation, or posterior pedicle screw fixation. Pedicle fixation is discussed elsewhere; so the primary focus of this transient dialogue is structural anterior interbody grafting and anterior vertebral fixation. Most anterior lumbar fixation constructs are variations on the rigid cantilever beam design. The screws are hooked up rigidly to longitudinal members, typically either a rod or a plate. Similar to the interbody grafts, the cantilever beam construct functions in distraction most of the time by resisting compressive forces. Because of its rigid attachment to the vertebrae, nevertheless, it additionally resists extension, axial rotation, and lateral bending. Ideally, the axial compressive forces (load) should be shared between the cantilever beam instrumentation and the interbody graft. If extreme pressure is borne by the instrumentation, the bone graft materials might resorb and a pseudarthrosis may result. The interbody graft or device should therefore be positioned under gentle compression. Care must be taken, nonetheless, if compression is directly applied to the instrumentation; significant ventrolateral compression can create a segmental kyphosis or scoliosis. Anterior lumbar instrumentation, including the use of appropriately sized and positioned grafts, can effectively appropriate some spinal deformities. Small grafts positioned within the ventral disk house or bigger lordotic grafts masking most of the vertebral finish plates can increase segmental lordosis and proper a relative or frank kyphosis. Correction of a lumbar scoliosis can be achieved through the position of small structural grafts in the concavity of the intervertebral disk spaces and compressing throughout lateral vertebral body screws. Proper graft choice and placement are essential in this scenario to avoid concurrently creating a relative lumbar kyphosis through ventral compression. A kyphoscoliosis or vital kyphotic deformity is a relative contraindication to an anterior-only correction procedure. Higher lumbar ranges could be exposed but considerable vessel retraction could additionally be required.
Treatment and prognosis depend on whether or not the analysis is solitary plasmacytoma or systemic multiple myeloma gastritis diet juicing buy generic prevacid 30 mg. Both situations are exquisitely radiosensitive, but patients with solitary plasmacytomas have considerably longer survival occasions xylitol gastritis generic 30 mg prevacid amex. As tumors of the axial skeleton and cranium base, chordomas constitute 1% to 2% of all skeletal sarcomas chronic gastritis joint pain quality prevacid 15 mg. More than 50% of those lesions are positioned within the lumbosacral region, 35% are in the clival area, and the rest are unfold all through the vertebral column. Chordomas are the commonest major neoplasm of the sacrococcygeal region and happen predominantly within the fifth and sixth decades of life. Age at presentation and en bloc resection are probably one of the best prognostic indicators for disease-free survival after surgery, with youthful patients having better prognoses. There is a fair distribution of tumor involvement amongst cervical, thoracic, and lumbosacral areas. Primary and secondary chondrosarcomas often arise in middleaged and older patients and present a predilection for men. Prognosis correlates with tumor extension and grade; sufferers with unresectable chondrosarcomas have a 5-year survival price of solely 20%. These lesions are distributed evenly all through the spine, but the vertebral physique is concerned in additional than 95% of cases. Radiologically, osteogenic sarcomas usually exhibit lytic and sclerotic areas, with cortical destruction and ossification in the tumor mass. Preoperative embolization, chemotherapy, and surgical extirpation with adjuvant radiotherapy are the current treatment modalities. The vertebral body is most often involved, and males are affected greater than females, at a ratio of 2: 1. Diagnosis relies on biopsy, and treatment entails a multidisciplinary approach combining surgical extirpation, radiation, and chemotherapeutic protocols. Younger sufferers are inclined to have a better prognosis; survival at 5 years approaches 75%. Intradural extramedullary tumors account for 40% to 50% of all spinal twine tumors, and extradural tumors account for 30%. Nerve sheath tumors, meningiomas, and filum terminale ependymomas are the most typical extramedullary spinal twine tumors, with nerve sheath tumors and meningiomas accounting for greater than 70% to 80%. Back pain is the most typical initial grievance in adults; youngsters with extramedullary tumors tend to present with neurological deficits within the form of motor or gait disturbances. Neurological compromise ensues as soon as maximal compliance of the encircling constructions is reached and compression is transmitted on to the spinal cord. Most extramedullary neoplasms produce local segmental deficits before a distant neurological deficit appears. Lumbosacral or conus medullaris lesions produce lower extremity weak point as properly as bladder and bowel signs. Most are schwannomas that happen proportionally all through the spinal canal, and most are entirely intradural. Ten % to 15% have both intradural and extradural parts, and approximately 10% are completely extradural. Most nerve sheath tumors come up from a dorsal nerve root; tumors arising from a ventral root usually have a tendency to be neurofibromas. Caudally located nerve sheath tumors could displace adjoining nerve roots and might erode the bone of nearby foramina as the neoplasm grows. Patients current with imprecise ache or localized backbone ache related to radicular ache and proof of nerve root or spinal twine impairment. Most common within the thoracic spine, meningiomas are the most common benign tumor at the foramen magnum. Most are intradural; nonetheless, roughly 10% are either intradural and extradural or totally extradural. The majority current between the fifth and seventh a long time of life, and more than 70% occur in girls. Clinical presentation is just like that of nerve sheath tumors, but with fewer radicular symptoms. These lesions account for approximately 15% of extramedullary spinal wire tumors, and approximately 40% of all spinal ependymomas come up throughout the proximal intradural filum. Radiation is reserved for biologically aggressive tumors, which are extra frequent within the younger inhabitants. The majority are intradural extramedullary tumors such as dermoids, epidermoids, lipomas, teratomas, and neuroenteric cysts that end result from disordered embryogenesis. Paragangliomas are uncommon tumors that may arise from the filum terminale or cauda equina. Hemangioblastomas and ganglioneuromas can involve intradural nerve roots and present as extramedullary mass lesions. Astrocytomas can happen at any age however are commonest in the first three a long time of life; they constitute 90% of intramedullary tumors in sufferers younger than 10 years and 60% of intramedullary tumors in adolescents. Approximately 90% of pediatric astrocytic tumors are benign fibrillary astrocytomas or juvenile pilocytic astrocytomas, whereas fibrillary astrocytomas prevail in adults. Astrocytic tumors typically infiltrate adjoining spinal twine tissue, however solely 10% of pediatric intramedullary astrocytomas are malignant, compared with 25% of grownup tumors. Both astrocytomas and ependymomas produce fusiform dilation of the spinal wire and are associated with low- to intermediate-intensity indicators on T1-weighted pictures and better signal intensity on T2-weighted images; ependymomas tend to have more marked enhancement, better outlined borders, and a extra central location. Adjuvant radiation therapy for glial tumors is controversial, and a few investigators have found no important benefit related to this remedy. Gangliogliomas, oligodendrogliomas, and neurocytomas are uncommon intramedullary glial-derived tumors. These lesions represent 20% to 25% of spinal cord tumors, and most are astrocytomas and ependymomas. Gangliogliomas, oligodendrogliomas, subependymomas, hemangioblastomas, neurocytomas, and metastases are a lot much less frequent. Children are predisposed to astrocytic tumors; nonetheless, ependymomas turn out to be extra widespread with age. Intramedullary spinal wire tumors manifest with insidious pain localized to the extent of the tumor, unrelated to mechanical exercise, and not relieved with relaxation. A neurological deficit is usually present at diagnosis, and the insidious onset of signs can delay prognosis for so lengthy as 2 years. The location of the intramedullary tumor dictates the evolution of the neurological deficit. Most intramedullary tumors produce local segmental and distant neurological deficits. Cervical segmental findings include weak spot, fasciculation, and atrophy of the hand muscles. Because of their central location, intramedullary spinal cord tumors may produce a central cord-like syndrome, with relative sparing of the extra radially located lumbosacral nerve tracts. Although related, these diseases symbolize two different pathologic situations with regard to sex, age, location, related scientific findings, immunologic characterization, and indications for surgical intervention. Neurological deficits are often a late manifestation of those chronic disease processes. The commonest skeletal manifestation is involvement of the metatarsophalangeal joints, followed by the cervical spine. Craniocervical instability from atlantoaxial subluxation is current in 19% to 70% of circumstances, and 20% of patients with atlantoaxial subluxation have some degree of basilar invagination. Basilar invagination is less common than atlantoaxial subluxation however is extra frequently associated with neurological deficits. Subaxial subluxation most often occurs at C2-3 and C3-4, producing a "staircase" appearance on imaging. Radiographic sequelae embrace delicate tissue swelling, narrowing of joint spaces, and in the end bone erosion, with deformity and instability. Surgical intervention for decompression with or with out fixation is warranted for myelopathy, progressive subluxation, and severe pain.






