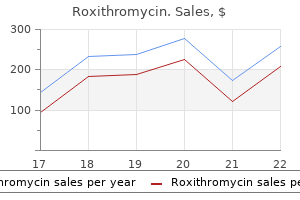
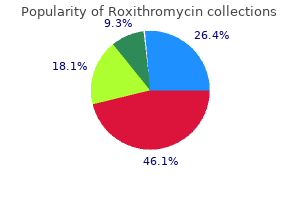
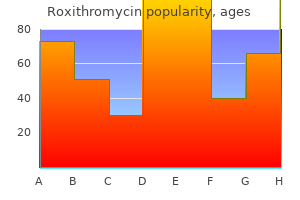
Roxithromycin
Roxithromycin
Roxithromycin dosages: 150 mg
Roxithromycin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Hemodialysis includes the diffusion of solutes across a semipermeable membrane between the blood and a dialysis solution antibiotics for acne solodyn purchase 150 mg roxithromycin with mastercard. This results in the removal of metabolic waste products and excess fluid quantity antibiotic keflex breastfeeding purchase roxithromycin 150 mg with amex, as well as the replenishment of body buffers antibiotic resistance hsc roxithromycin 150 mg generic on line. The dose of dialysis, kind of dialysis membrane, and solute clearance are crucial modifiable elements. The annual mortality for patients receiving hemodialysis is sort of 25% and is most often attributed to cardiovascular causes or infection. A surgically created vascular access web site is critical for efficient hemodialysis. Native arteriovenous fistulas (cephalic vein anastomosed to the radial artery) are superior to polytetrafluoroethylene grafts as websites of vascular entry due to their longer life span and lower incidence of thrombosis and an infection. The most typical accessrelated complication is intimal hyperplasia, which leads to stenosis proximal to the venous anastomosis. Other issues related to entry embody thrombosis, an infection, aneurysm formation, and limb ischemia. When dialysis is urgently required, vascular entry is obtained with a double-lumen dialysis catheter, most frequently using the jugular or femoral vein. Hypotension is the most typical antagonistic event during hemodialysis and most likely reflects osmolar shifts and ultrafiltration-induced volume depletion. Hypotensive episodes may be as a outcome of myocardial ischemia, cardiac dysrhythmias, or pericardial effusion Hemodialysis and Associated Clinical Challenges with cardiac tamponade. Most hypotensive episodes are efficiently handled by slowing the speed of ultrafiltration and/or administering intravenous saline. Hypersensitivity reactions to the ethylene oxide used to sterilize dialysis machines, in addition to antagonistic reactions to the specific hemodialysis membrane material polyacrylonitrile, might occur. Dialysis disequilibrium syndrome is marked by nausea, headaches, and fatigue, but could progress to seizures or coma. The situation is believed to outcome from fast changes in pH and solute concentrations in the central nervous system. Management includes reducing the speed of dialysate and blood flow and utilizing dialyzers with smaller floor space. Muscle cramps are a frequent complaint and most likely mirror adjustments in potassium concentrations. During progressive renal failure, catabolism and anorexia lead to lack of lean body mass, however concomitant fluid retention masks weight reduction and will even result in weight acquire. Decreased oral intake, hemodialysisinduced catabolism, and hormonal imbalances are frequent components. Amino acids in addition to water-soluble nutritional vitamins are eliminated by dialysis, which contributes to malnutrition. Routine evaluation of dietary status utilizing plasma biomarkers (albumin, prealbumin) is advised, and plenty of sufferers benefit from oral or parenteral nutritional dietary supplements. The expected cardiac and neuromuscular responses to hyperkalemia are much less pronounced in patients receiving hemodialysis than in these with normal renal operate. Patients should obtain counseling with regard to regulation of sodium and fluid consumption. Decreased catabolism of insulin in many sufferers receiving hemodialysis may result in decreased insulin requirements in contrast with wants before the initiation of hemodialysis. The presentation of diabetic ketoacidosis could additionally be atypical, with respiratory acidosis and alkalosis however without metabolic acidosis and hypovolemia. Contributing elements embrace impaired phagocytosis and neutrophil chemotaxis, and malnutrition. Tuberculosis in patients receiving hemodialysis is usually extrapulmonary and sometimes presents with atypical signs that mimic these of insufficient dialysis. Because anergy in response to pores and skin testing is common, unexplained weight reduction and anorexia, with or with out persistent fever, should immediate further testing to rule out tuberculosis. Hepatitis B or C virus an infection in sufferers receiving hemodialysis is usually asymptomatic, and liver aminotransferase concentrations may not be elevated. A substantial proportion of patients present process hemodialysis have antibodies to hepatitis C. Peritoneal dialysis requires inserting an anchored plastic catheter in the peritoneal cavity for infusion of a dialysate that remains in place for a quantity of hours. During that point, diffusive solute transport happens across the peritoneal membrane until contemporary fluid is exchanged for the old fluid. Automated peritoneal dialysis, during which a mechanized cycler infuses and drains peritoneal dialysate at evening, is used in many sufferers. Peritoneal dialysis may be desirable for sufferers with congestive coronary heart failure or unstable angina who might not tolerate the fast fluid shifts or fluctuations in systemic blood stress that always accompany hemodialysis. Peritoneal dialysis can also be indicated for sufferers with intensive vascular disease that stops the creation of a vascular access web site for hemodialysis. In patients with diabetes, insulin can be infused with the dialysate to provide exact regulation of blood glucose concentrations. The presence of stomach hernias or adhesions could intervene with the ability to use peritoneal dialysis successfully. Peritonitis presenting as belly pain and fever is the commonest severe complication of peritoneal dialysis. Treatment is with antibiotics, which can include cephalosporins, aminoglycosides, and vancomycin. Survival charges and annual prices are comparable with peritoneal dialysis and hemodialysis, but hospitalization charges are greater among sufferers handled with peritoneal dialysis. When attainable, drug doses are greatest scheduled for administration after completion of a dialysis session. Drug properties that influence clearance by dialysis include protein binding, water solubility, and molecular weight. Drug Clearance in Patients Undergoing Dialysis Peritoneal Dialysis Low-molecular-weight (<500 Da), water-soluble, nonproteinbound medicine are readily cleared by dialysis. Patients should undergo adequate dialysis inside 24 hours of elective surgery to minimize the chance of volume overload, hyperkalemia, and uremic bleeding. Depending on the deliberate surgical procedure, the usage of heparin could also be prevented or minimized during preoperative hemodialysis. Optimal management of modifiable danger components and the event of an anesthetic administration plan aimed toward minimizing further kidney harm are crucial. In addition to figuring out sufferers with preexisting renal dysfunction, it may be very important recognize those who are at excessive risk of developing perioperative renal failure. Evaluation of the pattern in serum creatinine focus is helpful to determine whether renal perform is stable. Blood quantity standing may be estimated by comparing physique weight earlier than and after hemodialysis, monitoring very important indicators (orthostatic hypotension, tachycardia), and measuring atrial filling pressures. Because diabetes is usually current in these sufferers, glucose management is of concern. Preoperative medication should be individualized, with recognition that these patients might exhibit sudden sensitivity to central nervous system depressant drugs. Attenuated sympathetic nervous system exercise impairs compensatory peripheral vasoconstriction; thus, small decreases in blood volume, institution of positive pressure air flow, abrupt modifications in physique position, or drug-induced myocardial despair can end result in an exaggerated lower in systemic blood strain. The preoperative presence of a coagulopathy could additionally be addressed with the administration of desmopressin. Gastric aspiration prophylaxis ought to be thought of, particularly in diabetic patients. However, all H2-receptor blockers are excreted renally; subsequently dosage adjustment is required. Patients maintained on dialysis ought to endure dialysis inside the 24 hours previous elective surgical procedure. The probability of hypotension is increased by uremia as nicely as by the administration of antihypertensives. Exaggerated central nervous system effects of anesthetic induction medication may also mirror uremia-induced disruption of the blood�brain barrier. If indicated, rapid-sequence induction with succinylcholine could additionally be carried out if the potassium focus is lower than 5. A balanced anesthetic method utilizing a volatile agent, muscle relaxant, and opioids is most often employed. Potent unstable anesthetics are helpful for controlling intraoperative systemic hypertension and lowering the doses of muscle relaxants needed for sufficient surgical rest.
Syndromes
In view of the skeletal muscle weakness gluten free antibiotics for sinus infection purchase roxithromycin 150 mg mastercard, there was concern that these sufferers could show irregular responses to muscle relaxants antibiotics diverticulitis roxithromycin 150 mg purchase amex. However antibiotics kill candida purchase roxithromycin 150 mg with amex, responses to nondepolarizing muscle relaxants and succinylcholine are regular in patients with polymyositis. Muscular Dystrophy Muscular dystrophy is a gaggle of hereditary diseases characterised by painless degeneration and atrophy of skeletal muscular tissues. There are progressive, symmetrical skeletal muscle weak point and wasting however no proof of skeletal muscle denervation. The disease is brought on by an X-linked recessive gene and becomes apparent in 2- to 5-year-old boys. Initial symptoms embody a waddling gait, frequent falling, and difficulty climbing stairs, and these replicate involvement of the proximal skeletal muscle teams of the pelvic girdle. Affected muscle tissue turn out to be larger on account of fatty infiltration, and this accounts for the designation of this disorder as pseudohypertrophic. There is progressive deterioration in skeletal muscle power, and usually these boys are confined to a wheelchair by age 8 to 10. Serum creatine kinase concentrations are 20 to 100 times normal, even early within the disease, reflecting increased permeability of skeletal muscle membranes and skeletal muscle necrosis. Approximately 70% of the female carriers of this disease additionally exhibit increased serum creatine kinase concentrations. Skeletal muscle biopsy specimens early in the course of the illness may show necrosis and phagocytosis of muscle fibers. Death usually occurs at 15 to 25 years of age as a end result of congestive coronary heart failure and/or pneumonia. Mitral regurgitation might happen because of papillary muscle dysfunction or decreased myocardial contractility. Chronic weakness of the respiratory muscle tissue and a weakened cough end in loss of pulmonary reserve and accumulation of secretions. Respiratory insufficiency usually stays covert as a end result of overall exercise is so restricted. As the illness progresses, kyphoscoliosis contributes to additional restrictive lung disease. Sleep apnea could occur and may contribute to improvement of pulmonary hypertension. Approximately 30% of deaths in individuals with pseudohypertrophic muscular dystrophy are due to respiratory causes. Children with pseudohypertrophic muscular dystrophy may require anesthesia for muscle biopsy or correction of orthopedic deformities. Preparation for anesthesia must take into consideration the implications of elevated skeletal muscle membrane permeability and decreased cardiopulmonary reserve. Hypomotility of the gastrointestinal tract could delay gastric emptying and, within the presence of weak laryngeal reflexes, can increase the risk of pulmonary aspiration. Management of Anesthesia Use of succinylcholine is contraindicated because of the risk of rhabdomyolysis, hyperkalemia, and/or cardiac arrest. Indeed, ventricular fibrillation during induction of anesthesia that included succinylcholine administration has been noticed in sufferers later found to have this form of muscular dystrophy. Rhabdomyolysis, with or with out cardiac arrest, has been observed in affiliation with administration of volatile anesthetics to these patients even in the absence of succinylcholine administration. Malignant hyperthermia has been noticed after even brief durations of halothane administration, although most cases have been triggered by succinylcholine or prolonged inhalation of halothane. Regional anesthesia avoids the unique dangers of general anesthesia in these patients. During the postoperative interval, neuraxial analgesia could facilitate chest physiotherapy. Monitoring is directed at early detection of malignant hyperthermia and cardiac depression. Postoperative pulmonary dysfunction ought to be anticipated and attempts made to facilitate clearance of secretions. Delayed pulmonary insufficiency may occur up to 36 hours postoperatively although skeletal muscle energy has apparently returned to its preoperative ranges. Early symptoms embody problem elevating the arms above the top and problem smiling. Recovery from atracurium-induced neuromuscular blockade could also be quicker than regular in these sufferers. Histologic examination demonstrates the presence of rods between regular myofibrils. Affected people expertise delayed motor growth, generalized skeletal muscle weak spot, a lower in muscle mass, hypotonia, and loss of deep tendon reflexes. Affected infants may present with hypotonia, dysphagia, respiratory distress, and cyanosis. Tracheal intubation could also be difficult due to anatomic abnormalities corresponding to micrognathia and a high-arched palate. The respiratory depressant effects of medicine may be exaggerated in these sufferers due to respiratory muscle weak point and chest wall abnormalities. Ventilation/perfusion mismatching is increased, and the ventilatory response to carbon dioxide may be blunted. Bulbar palsy related to regurgitation and aspiration could further complicate anesthetic management. The response to succinylcholine and nondepolarizing neuromuscular blockers is unpredictable. Malignant hyperthermia has not been reported in patients with nemaline rod myopathy. Myocardial depression might accompany administration of unstable anesthetics if the disease course of involves the myocardium. Plans for regional anesthesia should contemplate the attainable respiratory compromise that could accompany a high motor block. In addition, the exaggerated lumbar lordosis and/or kyphoscoliosis might make neuraxial anesthesia technically tough. Electromyographic findings are diagnostic and are characterized by prolonged discharges of repetitive muscle motion potentials. Intracellular adenosine triphosphatase fails to return calcium to the sarcoplasmic reticulum, so unsequestered calcium remains out there to produce sustained skeletal muscle contraction. Infiltration of contracted skeletal muscular tissues with local anesthetic could induce rest. Increasing the ambient temperature of the working room decreases the severity of myotonia and the incidence of postoperative shivering, which may precipitate skeletal muscle contraction. Although expertise is limited, these sufferers may be vulnerable to aspiration through the perioperative period, and their sensitivity to muscle relaxants could also be increased. Cardiac involvement may be life-threatening and present as congestive heart failure, thromboembolism, or bradycardia. Unlike in different muscular dystrophies, feminine carriers of this disorder could experience cardiac impairment. Myotonia dystrophica is the commonest and most severe form of myotonic dystrophy affecting adults. It is inherited as an autosomal dominant trait, with the onset of signs during the second or third decade. Unlike different myotonic syndromes, myotonia dystrophica is a multisystem disease, although skeletal muscles are affected most. This reflects progressive involvement of skeletal muscle, cardiac muscle, and clean muscle. Perioperative morbidity and mortality charges are high principally because of cardiopulmonary issues. Quinine and procainamide also have antimyotonic properties however can worsen cardiac conduction abnormalities. These three medicine depress sodium influx into skeletal muscle cells and delay the return of membrane excitability.
The antibodies might activate endothelial cells to improve the expression of vascular adhesion molecule 1 and E-selectin antibiotic lock therapy idsa cheap roxithromycin 150 mg free shipping. This would improve the binding of white blood cells and platelets to the endothelial surface and lead to antibiotics medicine 150 mg roxithromycin purchase thrombus formation antibiotics for sinus infection uk order roxithromycin 150 mg online. Patients with lupus anticoagulants have an increased propensity for thrombosis, with 30% to 60% of sufferers experiencing a quantity of thrombotic events throughout their lifetime. Isolated venous thrombosis or thromboembolism make up two thirds of the events and cerebral thrombosis accounts for the opposite third. Along with issue V Leiden and the prothrombin gene mutation, the presence of an antiphospholipid antibody must be considered as a likely reason for thromboembolic disease in youthful people. Hyperlipidemia and hypoalbuminemia have additionally been proposed as potential etiologic factors. Management of Anesthesia in Venous Hypercoagulable Disorders Current antithrombotic strategies range from easy administration approaches such as early ambulation to a mixture of elastic stockings and subcutaneous heparin remedy adopted by conversion to outpatient warfarin therapy. Recent meta-analyses have discovered that regional and general anesthesia for hip surgical procedure appear to produce comparable outcomes by means of most outcomes. Food and Drug Administration advisory prohibiting neuraxial anesthesia in patients receiving low-molecular-weight heparin ensuing from an elevated threat of epidural hematomas may additional restrict the usage of regional anesthesia or its extension into the postoperative interval. Patients with an absolute contraindication to anticoagulant therapy or those with a significant bleeding complication may profit from placement of a vena caval filter to prevent recurrent pulmonary emboli. The filters are efficient and reduce the incidence of pulmonary embolism to lower than 4%. In cancer patients for whom anticoagulant remedy has failed, a vena caval filter combined with continued anticoagulation might provide higher protection. Perioperative administration of patients receiving anticoagulant remedy requires special consideration. Certain operations such as some ophthalmic, dental, dermatologic, and gastrointestinal procedures may be carried out with out interruption of oral anticoagulant therapy. The danger of perioperative thrombosis should be weighed towards the danger of bleeding throughout and after surgical procedure. For most operations anticoagulation must be briefly interrupted, and bridging remedy with unfractionated or low-molecular-weight heparin is instituted in sufferers at reasonable and excessive threat of thrombosis. Warfarin must be stopped roughly 5 days before the process and heparin must be began 36 hours after the final dose of warfarin. In circumstances by which neuraxial anesthesia is deliberate, the rules of the American Society of Regional Anesthesia and Pain Medicine recommend that needle placement for regional anesthesia take place 12 hours after the last dose of low-molecular-weight heparin if prophylactic dosing is used and 24 hours after the final dose of low-molecular-weight heparin if therapeutic dosing is used. Similarly, epidural catheter removing needs to be fastidiously coordinated with the heparin dosing (Table 20-7). Resumption of anticoagulation postoperatively requires an evaluation of the risk of recurrent thrombosis and consideration of the diploma to which surgery itself increases hypercoagulability. These elements have to be weighed towards the bleeding danger associated with resumption of anticoagulation. These sufferers could be managed with bridging therapy with heparin till the worldwide normalized ratio reaches therapeutic ranges. Consider delaying heparin dose until after block if technical problem is anticipated. Twice-daily dosing: Delay neuraxial block for no much less than 24 hr after final preoperative dose of heparin. Once-daily dosing: Delay neuraxial block for at least 12 hr after last preoperative heparin dose. Use neuraxial blockade only if it might be accomplished with a single pass of an atraumatic needle and without an indwelling catheter. Patients with atrial fibrillation, significantly atrial fibrillation related to valvular illness, a dilated atrium, and evidence of heart failure or a prior embolus typically require moderatedose warfarin therapy indefinitely. In patients with atrial fibrillation undergoing main surgery, oral anticoagulant remedy must be stopped and bridging remedy with heparin begun. It is sometimes recommended that dabigatran be stopped three to 5 days earlier than surgery in sufferers with impaired renal operate (creatinine clearance <50 mL/min) and a pair of to 3 days earlier than surgical procedure in others. If parenteral anticoagulant therapy is critical, it should be initiated 12 to 24 hours after the final dose of dabigatran. Regional anesthesia in the affected person receiving antithrombotic or thrombolytic remedy: American Society of Regional Anesthesia and Pain Medicine EvidenceBased Guidelines (third edition). The perioperative management of antithrombotic therapy: American College of Chest Physicians EvidenceBased Clinical Practice Guidelines (8th edition). New heritable causes of hypercoagulability are being identified, and some genetic predisposition to thrombosis can be recognized in more than half of sufferers with deep vein thrombosis. Anesthesiologists are being requested to look after an growing variety of sufferers carrying the analysis of hypercoagulability, a lot of whom are receiving long-term anticoagulation therapy. Some surgeries are associated with a more than 100-fold increase in the danger of thrombosis. Hypercoagulability performs a less clearly outlined function within the pathophysiology of arterial thrombotic occasions, however the high morbidity and mortality associated with arterial occlusion in the perioperative patient makes staying abreast of those developments an important a half of affected person care. Preoperative management of patients with sickle cell illness now not mandates change transfusion to decrease the ratio of sickle Hb to regular Hb; as an alternative, transfusions are required solely as needed to obtain a preoperative hematocrit of 30%. Recent advances in cell-based coagulation fashions have modified our basic understanding of in vivo clotting. This improved understanding has allowed a better appreciation of how particular defects in coagulation components have an result on the steadiness of hemostasis and what therapeutic interventions provide the best risk/benefit ratio. Most issues producing a state of venous hypercoagulability have an effect on the era or disposition of thrombin, whereas in the arterial circulation, platelet and endothelial operate and regulation also critically affect the prothrombotic tendency. Annual medical updates in hematological malignancies: polycythemia vera and essential thrombocythemia: 2011 replace on diagnosis, riskstratification, and administration. The 4Ts scoring system for heparin-induced thrombocytopenia in medical-surgical intensive care unit patients. Clinical options of heparin-induced thrombocytopenia together with danger elements for thrombosis. However, less visible systemic results of many of these disorders are also essential. In the simplex sort, epidermal cells are fragile because of mutations of genes encoding keratin intermediate filament proteins. The simplex type of epidermolysis bullosa has a benign course and growth is normal. By contrast, sufferers with the junctional type of epidermolysis bullosa rarely survive beyond early childhood. Features that distinguish junctional epidermolysis bullosa from different varieties are generalized blistering beginning at start, absence of scar formation, and generalized mucosal involvement (gastrointestinal, genitourinary, respiratory tracts). Manifestations of epidermolysis bullosa dystrophica embrace extreme scarring with fusion of the digits (pseudosyndactyly), constriction of the oral aperture (microstomia), and esophageal stricture. Malnutrition, anemia, electrolyte derangements, and hypoalbuminemia are frequent, most probably reflecting chronic an infection, debilitation, and renal dysfunction. Diseases related to epidermolysis bullosa embrace porphyria, amyloidosis, multiple myeloma, diabetes mellitus, and hypercoagulable states. Infection of bullae with Staphylococcus aureus or -hemolytic streptococci is frequent. Bulla formation may be brought on by trauma from tape, blood pressure cuffs, tourniquets, adhesive electrodes, and rubbing of the skin with alcohol wipes. Intravenous and intraarterial catheters ought to be sutured or held in place with gauze wraps somewhat than tape. Trauma from the anesthetic face mask should be minimized by light application in opposition to the face. Lubrication of the face and masks with cortisol ointment or another lubricant can be useful. Upper airway instrumentation ought to be minimized, as a result of the squamous epithelium lining the oropharynx and esophagus could be very prone to trauma. Frictional trauma to the oropharynx, corresponding to that produced by an oral airway, may end up in formation of enormous intraoral bullae and/or intensive hemorrhage from denuded mucosa. Hemorrhage from ruptured oral bullae has been handled successfully by application of epinephrine-soaked gauze on to the bullae. Interestingly, endotracheal intubation has not been related to laryngeal or tracheal complications in patients with epidermolysis bullosa dystrophica.
Lymphomas and leukemias are examples of cancers that contain the lymph glands and blood-forming parts antibiotics for esbl uti roxithromycin 150 mg order visa. Metastatic cardiac involvement-usually from adjoining lung cancer-occurs 20 to forty occasions extra typically than major malignant cardiac tumors antibiotics for uti how long does it take to work cheap 150 mg roxithromycin free shipping. About three quarters of cardiac myxomas happen in the left atrium antibiotic 93 3160 150 mg roxithromycin order, and the remaining 25% occur in the best atrium. Myxomas often reveal appreciable movement throughout the cardiac chamber in the course of the cardiac cycle. Signs and signs of cardiac myxomas replicate interference with filling and emptying of the involved cardiac chamber. Left atrial myxoma might mimic mitral valve illness with growth of pulmonary edema. Right atrial myxoma typically mimics tricuspid disease and could be related to impaired venous return and evidence of right-sided coronary heart failure. These emboli are composed of myxomatous material or thrombi that have fashioned on the tumor. Because most myxomas are situated in the left atrium, systemic embolism is particularly frequent and sometimes involves the retinal and cerebral arteries. Echocardiography can determine the situation, measurement, form, attachment, and mobility of cardiac myxomas. After the prognosis has been established, prompt surgery is indicated because of the potential of embolic problems and sudden dying. All chambers of the heart are examined to rule out the existence of multifocal illness. Mechanical harm to a coronary heart valve or adhesion of the tumor to valve leaflets might necessitate valvuloplasty or valve replacement. Preoperative evaluation includes a review of potential opposed results associated to chemotherapy. Placement of intravenous catheters in the arm susceptible to lymphedema is avoided due to the potential to exacerbate lymphedema and the susceptibility to infection. The presence of a proper atrial myxoma prohibits placement of proper atrial or pulmonary artery catheters. In some sufferers, permanent cardiac pacing could also be required due to atrioventricular conduction abnormalities. External beam radiation can be used for palliative therapy of obstructive and bony metastases. Esophageal Cancer Esophageal cancer has two histologic subtypes: squamous cell and adenocarcinoma. Excessive alcohol consumption and long-term cigarette smoking are impartial risk elements for the event of squamous cell carcinoma of the esophagus. Dysphagia and weight reduction are the preliminary symptoms of esophageal most cancers in most sufferers. Difficulty swallowing may lead to regurgitation and increase the danger of aspiration. The lack of a serosal layer across the esophagus and the presence of an extensive lymphatic system are liable for the rapid spread of tumor to adjacent lymph nodes. Even with aggressive remedy, the 5-year survival price for sufferers with squamous cell carcinoma is simply 15% to 20%. Esophagectomy is usually carried out for carcinoma of the esophagus and is related to important morbidity and mortality. Chemotherapy and radiation therapy may be instituted before surgical resection is attempted. Adenocarcinomas are radioinsensitive, however chemotherapy and surgery might improve survival. Palliation might embrace surgical placement of a feeding tube, bougienage, or endoscopic stent placement. The probability of underlying alcohol-induced liver disease, continual obstructive pulmonary illness from cigarette smoking, and cross-tolerance of anesthetic drugs in patients who abuse alcohol are concerns during anesthetic management of patients with esophageal most cancers. Extensive weight reduction often parallels a decrease in intravascular fluid quantity and manifests as hypotension during induction and maintenance of anesthesia. Head and Neck Cancers Head and neck cancers account for roughly 5% of all cancers in the United States, with a predominance in men older than 50 years of age. Hypercalcemia may be related to bony metastases, and altered liver perform check outcomes presumably replicate alcohol-induced illness. The goal of chemotherapy, if chosen, is to lower the majority of the primary tumor or recognized metastases and thereby improve the efficacy of subsequent surgical procedure or radiation treatment. Anesthetic issues in patients with head and neck cancers embody the potential of distorted airway anatomy that will not be appreciated on external airway examination. Available diagnostic photographs and the report of nasal fiberoptic examination should be reviewed preoperatively. Preparation must be made for the potential for difficult ventilation and/ or intubation. Thyroid Cancer Papillary and follicular thyroid carcinomas are among the many most curable of all cancers. External radiation to the neck throughout childhood increases the chance of papillary thyroid cancer, as does a family history of the illness. This type of thyroid cancer sometimes produces massive amounts of thyrocalcitonin, which provides a sensitive measure of the presence of the illness as properly as its successful remedy. Subtotal and total thyroidectomy lead to decrease recurrence rates than extra limited partial thyroidectomy. Even with total thyroidectomy, some thyroid tissue stays, as detected by postoperative scanning with radioactive iodine. Risks of total thyroidectomy embrace recurrent laryngeal nerve damage (2%) and everlasting hypoparathyroidism (2%). Patients with papillary thyroid cancers require dissection of paratracheal and tracheoesophageal lymph nodes. The development of papillary and follicular tumor cells is managed by thyrotropin, and inhibition of thyrotropin secretion with thyroxine improves Gastric Cancer the incidence of gastric cancer has decreased dramatically since 1930, when it was the main explanation for cancer-related death among males within the United States. Achlorhydria (loss of gastric acidity), pernicious anemia, continual gastritis, and Helicobacter an infection contribute to the event of gastric cancer. The presenting features of gastric most cancers (indigestion, epigastric misery, anorexia) are indistinguishable from these of benign peptic ulcer illness. Approximately 90% of gastric cancers are adenocarcinomas, and approximately half of them occur within the distal portion of the stomach. Gastric cancer is often far advanced when signs and symptoms such as weight loss, palpable epigastric mass, jaundice, and ascites appear. Gastric most cancers is comparatively resistant to radiation remedy, but it is among the few gastrointestinal tumors which will have some response to chemotherapy. Liver Cancer Liver cancer happens most often in males with liver disease caused by hepatitis B or hepatitis C virus, alcohol consumption, or hemochromatosis. Initial manifestations are typically stomach pain, palpable stomach mass, and constitutional symptoms such as anorexia and weight loss. There could also be compression of the inferior vena cava and/or portal vein, lower extremity edema, ascites, and jaundice. Laboratory findings reflect the abnormalities related to underlying persistent liver disease. Celiac plexus block with alcohol or phenol is the simplest intervention for treating the pain associated with pancreatic cancer. A complication of celiac plexus block is hypotension resulting from sympathetic denervation in these often hypovolemic patients. Renal Cell Cancer Renal cell most cancers most frequently manifests as hematuria, mild anemia, and flank pain. The solely healing treatment for renal cell carcinoma confined to the kidneys is radical nephrectomy with regional lymphadenectomy. Pancreatic Cancer Pancreatic cancer, regardless of its low incidence, is the fourth commonest reason for cancer-related death in women and men in the United States. Approximately 95% of pancreatic cancers are ductal adenocarcinomas, with most occurring within the head of the pancreas. Jaundice reflects biliary obstruction in patients with tumor within the head of the pancreas. Pancreatic most cancers could appear as a localized mass or as diffuse enlargement of the gland. Patients more than likely to have resectable lesions are these with tumors within the head of the pancreas that trigger painless jaundice.
Diseases Associated with Obesity Obesity can have detrimental results on many organ systems oral antibiotics for moderate acne 150 mg roxithromycin quality. The most profound results are on the endocrine bacteria pictures roxithromycin 150 mg cheap on-line, cardiovascular antibiotic resistance presentation roxithromycin 150 mg cheap visa, respiratory, gastrointestinal, immune, musculoskeletal, and nervous systems. Clinically severely overweight people have limited mobility and should due to this fact appear to be asymptomatic even in the presence of great respiratory and cardiovascular impairment. Many of the comorbid situations brought on by obesity are associated to the metabolic syndrome, also identified as syndrome X. In sufferers with clinically extreme obesity, cardiac operate is greatest at relaxation and exercise is poorly tolerated. Any enhance in cardiac output is achieved by an increase in heart rate with out an increase in stroke volume or ejection fraction. Changing place from sitting to supine is related to a rise in pulmonary capillary wedge pressure and mean pulmonary artery stress in addition to a decrease in coronary heart price and systemic vascular resistance. Obese individuals with cardiac dysfunction could choose to sleep sitting up in a chair to avoid symptoms of orthopnea and paroxysmal nocturnal dyspnea. Mild to moderate systemic hypertension is three to six occasions extra frequent in obese than in lean sufferers and is seen in approximately 50% to 60% of overweight patients. Obesity-induced hypertension is expounded to insulin effects on the sympathetic nervous system and extracellular fluid volume. Hyperinsulinemia seems to enhance circulating ranges of norepinephrine; norepinephrine has direct pressor exercise and will increase renal tubular reabsorption of sodium and calcium, which finally ends up in hypervolemia. Cardiac output will increase by an estimated one hundred mL/min for each kilogram of adipose tissue weight gain. At the mobile degree, insulin activates adipocytes to release angiotensinogen, which prompts the renin-angiotensin-aldosterone pathway; this in turn results in sodium retention and improvement of hypertension. An improve in circulating cytokines is seen in weight problems, and this will trigger injury to and fibrosis of the arterial wall, thereby growing arterial stiffness. In common, a decrease of 1% in physique weight can lower systolic blood pressure by 1 mm Hg and diastolic blood pressure by 2 mm Hg. Obesity seems to be an impartial threat factor for the event of ischemic heart illness, and this coronary artery illness is more common in obese people with central (abdominal) fats distribution. This threat is compounded by the presence of dyslipidemia, a chronic inflammatory state, hypertension, and diabetes mellitus. Insulin resistance and irregular glucose tolerance are related to progression of atherosclerosis. Young obese patients are exhibiting a big incidence of single-vessel coronary artery illness, notably in the best coronary artery. Obese men appear to be affected 10 to 20 years before ladies, which may mirror a protecting impact from estrogen that dissipates after menopause. Possible mechanisms for the event of this coronary heart failure are structural and functional modifications of the guts ensuing from volume overload and vascular stiffness. These modifications in obese sufferers trigger stress overload that leads to concentric left ventricular hypertrophy, a progressively much less compliant left ventricle, left ventricular diastolic dysfunction, and, finally, left ventricular systolic dysfunction. Increased metabolic demands and a larger circulating blood quantity result in a hyperdynamic circulation. Insulin resistance additionally appears to play a big role within the development of heart failure. Cardiac steatosis, lipoapoptosis, and activation of particular cardiac genes that promote left ventricular remodeling and cardiomyopathy might contribute to obesity-related cardiomyopathy. The increased demands placed on the cardiovascular system by obesity lower cardiovascular reserve and limit train tolerance. Cardiac dysrhythmias in obese people could also be precipitated by arterial hypoxemia, hypercarbia, ischemic coronary heart disease, obesity hypoventilation syndrome, and fatty infiltration of the cardiac conduction system. It is essential to observe that ventricular hypertrophy and dysfunction worsen with the period of weight problems. However, a few of these structural and useful modifications are reversible with vital weight reduction. Obesity can produce an extrinsic restrictive sample of ventilation ensuing from the added weight of the thoracic cage or chest wall and stomach. This ends in ventilation/perfusion mismatching, right-to-left intrapulmonary shunting, and arterial hypoxemia. Obese people are likely to expertise oxygen desaturation following induction of anesthesia regardless of sufficient preoxygenation. To keep normocapnia, overweight sufferers must enhance minute air flow, which also increases the work of respiratory. Obese patients will typically enhance their minute ventilation by rapid shallow respiratory, as a result of this respiration sample utilizes the least quantity of power and may forestall fatigue from the elevated work of respiration. Clinically severely obese people might exhibit solely modest decreases in arterial oxygenation and modest increases within the alveolar-arterial oxygen distinction. The Paco2 and ventilatory response to carbon dioxide remain inside the normal range in obese patients, which displays the high diffusing capacity and favorable characteristics of the carbon dioxide dissociation curve. The lower in lung compliance is caused by accumulation of fats tissue in and across the chest wall and abdomen and the added effects of increased pulmonary blood quantity. These changes in lung compliance and resistance are most marked when obese individuals assume the supine position. Hypopnea is a discount in the dimension or variety of breaths in contrast with regular air flow and is associated with some extent of arterial desaturation. Pharyngeal patency is decided by the motion of dilator muscular tissues that prevent upper airway collapse. The pharyngeal muscle tone is decreased throughout sleep, and in many people, this lowered tone results in a significant narrowing of the higher airway, leading to turbulent airflow and snoring. In susceptible individuals this may progress to extreme loud night breathing and, in the end, to sleep apnea. Sleep fragmentation is the most likely rationalization for the daytime somnolence, which is related to impaired focus, memory problems, and even motorized vehicle accidents in patients with sleep apnea. Airway obstruction may induce physiologic changes that embrace arterial hypoxemia, arterial hypercarbia, polycythemia, systemic hypertension, pulmonary hypertension, and right ventricular failure. In addition, patients could complain of morning headaches attributable to nocturnal carbon dioxide retention and cerebral vasodilation. Other components corresponding to night alcohol consumption or use of pharmacologic sleep aids can worsen the problem. Patients treated with positive airway pressure show improved neuropsychiatric function and a lessening of daytime somnolence. Nocturnal oxygen remedy is one other risk for individuals who experience vital oxygen desaturation. In extreme cases of sleep apnea surgical therapy, including uvulopalatopharyngoplasty, tracheostomy, or maxillofacial surgical procedure. It is characterised by nocturnal episodes of central apnea (apnea with out respiratory efforts) reflecting progressive desensitization of the respiratory center to nocturnal hypercarbia. Abnormal liver operate take a look at results and fatty infiltration of the liver are frequent findings. Therefore, warning must be used when selecting medicines identified to trigger liver dysfunction. Interestingly, the elevated metabolism of volatile anesthetics (defluorination) seen in overweight patients has not been proven to end in hepatic dysfunction. Obesity causes an excess of intrahepatic triglycerides, impaired insulin exercise, and extra release of inflammatory cytokines. These components can lead to destruction of hepatocytes and disruption of hepatic physiology and structure. Approximately one third of overweight kids, adolescents, and adults have nonalcoholic steatohepatitis. However, in extreme instances it might progress to cirrhosis, portal hypertension, and/or hepatocellular carcinoma requiring liver transplantation. Most sufferers are asymptomatic, but some may expertise fatigue and abdominal discomfort. Most commonly, obese sufferers have cholelithiasis ensuing from supersaturation of bile with cholesterol ensuing from irregular ldl cholesterol metabolism.
Arrow Bamboo (Bamboo). Roxithromycin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96581
Specimens for cytological examination could also be obtained by the following strategies: Culture Whenever urinary dipstick evaluation or the clinical picture suggests a urinary an infection antibiotic synonym best 150 mg roxithromycin, then routine culture and sensitivities should be undertaken 15 antimicrobial drugs buy cheap roxithromycin 150 mg line. Adequate information have to be supplied on the request type infection gums buy cheap roxithromycin 150 mg on-line, particularly whether the affected person has obtained antibiotics in the latest past. Any cultured microbial growth ought to be subjected to antibiotic sensitivity studies. Preliminary tradition results may take 24 and even forty eight hours if anaerobic organisms are current. Catheter-related sepsis is usually related to microbial colonization of an indwelling urinary catheter. In the past, the one means of distinguishing between true catheter colonization and clinically insignificant contamination was by removing the catheter and culturing the tip. An endoluminal brush technique, passing a nylon brush down the lumen of the catheter to its tip and then culturing the comb end, can keep away from the unnecessary removal on noncolonized catheters. Touch, brush and fantastic needle aspiration sample preparations can be instantly smeared on to slides and air-dried or positioned into an appropriate transport medium and spun down later. It is sensible to leave the slide preparation to the cytopathology laboratory employees, as the higher the preparation the more accurate the interpretation. These examples are given to stress the significance of a close liaison between the clinician and the cytopathologist working together inside a multidisciplinary team. Histology the histological examination of a piece of tissue allows the examination not only of its cells but in addition the character and structure of the tissues around it. A fantastic needle aspiration being performed on a breast lump utilizing a 21 gauge needle and a 10-mL syringe however particular stains could additionally be more acceptable relying on the initial appearances. The reporting of the abnormalities seen in cytology specimens and their medical interpretation should be unambiguous. For instance, in the case of breast biopsies they should be reported as: inadequate benign in all probability benign suspicious for malignancy diagnostic of malignancy C1 C2 C3 C4 C5 needle biopsy. Similarly, thyroid specimens must be reported as: non-diagnostic � unsuitable for prognosis non-neoplastic, i. The samples the pathologist takes from the specimen are mounted, embedded in paraffin, sliced after which stained. The histological examination of an operative specimen can set up a proper analysis and confirm the adequacy of the therapeutic surgical procedure. In many instances an excision biopsy will each establish 10 Principles and strategies of investigation (A) about prognosis and can also point out whether or not further therapy is required. Special staging classifications also exist for circumstances such as lymphoma and melanoma. Special histological techniques Frozen part is used when a surgeon wants pressing pathological data during an operation. This can be provided by the histological examination of an immediately frozen piece of tissue taken through the operation. The want for this service is diminishing as a outcome of higher preoperative prognosis and as staging improves however when wanted should be arranged before the operation in consultation with the pathologist. Microscopical examination of surgically excised specimens of most cancers will often present data from which an correct staging may be deduced. Staging of any condition, which can also require the radiological evaluation of the presence of any distant metastatic unfold, supplies necessary information leukaemia/lymphoma classification muscle biopsies. Endoscopes may be introduced by way of natural orifices into the abdomen, colon, bronchi, urinary bladder and ureters, and nostril, throat and larynx. Most of those methods utilize versatile endoscopes that rely upon versatile fibreoptics. Others such as routine laparoscopy, thoracoscopy, arthroscopy and sigmoidoscopy are usually performed with rigid scopes however use fibreoptic light sources. In many instances an endoscopic technique can be used for both sampling and remedy. Their software to particular issues and illnesses is described within the related chapters. Rigid endoscopes encompass a central collection of rod lenses which transmit mild from the image to an eyepiece and provide a magnified view of the organ being noticed. Laparoscopes are available with angles of view of 0, 30 and 45 degrees and cystoscopes and sinoscopes can have a viewing angle of as a lot as one hundred twenty degrees. Surrounding the lens system is a sheath of fibreoptic glass fibres that transmit mild from the sunshine source to illuminate the cavity or organ under view. Flexible endoscopes comprise a bundle of flexible fibreoptic fibres that transmit the image either to an eyepiece or to a microchip video-camera from the place the picture is transmitted electronically to a television monitor/screen. Illumination is supplied from an intense mild supply, and the sunshine is transmitted through adjacent optical fibres included inside the sheath of the scope. Most endoscopes have a working channel via which devices may be handed corresponding to biopsy forceps, diathermy snares, Dormia baskets, stents and balloon catheters. Most versatile endoscopes are managed by rotating levers that enable the tip to be manipulated up and down, proper and left. It takes a substantial time to advance the scope down into the small bowel and, even then, very hardly ever offers a complete view of the bowel. This investigation is, to a level, operator dependent however skilled colonoscopists are often in a position to reach the caecum and even enter the terminal ileum. It is the investigation of alternative when looking for the source of bleeding such as angiodysplasia. If an obstructing tumour is encountered, a plastic stent or an expandable steel stent can be inserted. The intrabiliary stress may be Laparoscopy Diagnostic laparoscopy has been used for years by gynaecologists but its use has turn out to be increasingly popular with basic surgeons over the last 20 years. Some of the instruments that can be utilized via an endoscope: a Dormia basket, a sphicterotome, a cannula, biopsy graspers and a biopsy brush Endoscopic techniques 13 Although nearly all of laparoscopic procedures are now therapeutic operations, diagnostic laparoscopy continues to be a valuable investigation for the staging of tumours, biopsy of peritoneal or liver metastases and the evaluation of pelvic pathology, especially in younger female sufferers with lower abdominal ache (see Chapter 17). Cystoscopy Rigid cystoscopy for diagnostic and some therapeutic procedures has been in use for lots of a long time. It is feasible to acquire a safe and painless view of the entire of the lower urinary tract in both male and female patients inside an hour or so of presentation, within the outpatient division, utilizing native anaesthesia, and to take biopsies, resect small bladder tumours, visualize the upper urinary tracts radiologically, catheterize the ureters and insert or remove stents. Formal transurethral endoscopic resection of enormous tumours and prostatectomy utilizing diathermy loops, snares, knives or roller-balls nonetheless require common anaesthesia. Small calibre ureteroscopes now make it attainable to visualize the lumen of the ureter and the whole upper urinary tract and use laser lithotripsy, ultrasonic probes and fine basket catheters for the extraction of ureteric stones. The use of methods that fragment stones allows the removal of large calculi by this route. The therapeutic applications embody biopsy, bronchial lavage to take away extreme secretions, laser therapy to resect or debulk endobronchial tumours, and the insertion of stents (see Chapter 14). It is wise to obtain a clotting screen before subjecting a affected person to a bronchoscopy. Bronchoscopy might sometimes cause a minor deterioration of respiratory operate, a slight fever or pneumonia. Thoracoscopy Thoracoscopy permits intrathoracic diagnostic and therapeutic procedures to be carried out without having to resort to open thoracotomy. The lateral approach provides a greater view of the lungs while the susceptible strategy gives a better view of the mediastinum and for performing operative procedures on the sympathetic chain. The process is facilitated by the anaesthetist using a double lumen endotracheal tube, which enables the lungs to be selectively collapsed. Arthroscopy offers a wonderful view of any intra-articular disease process and, as with other endoscopic methods, enables therapeutic procedures to be carried out. Smaller endoscopes are available for the more distal joints of the upper and decrease limbs. Fluid irrigation is required to distend the joint, and a extensive range of devices similar to probes, intra-articular scissors, graspers, basket forceps, bone burrs and cautery have been designed to facilitate surgical procedures such as: biopsy synovectomy chondroplasty elimination of unfastened our bodies meniscectomy ligament repairs remedy of osteochondritis dissecans drainage of septic arthritis removing of osteoarthritic debris. When an ultrasonic wave strikes an interface between tissues with totally different acoustic impedance, some of the waves are mirrored and could be detected by a receiver consistent with the generator transmitting the waves. High frequency ultrasound can be used to monitor the development of sure pathological processes. The change in the frequency of an ultrasound wave mirrored from a transferring red cell is directly related to the rate of motion of the cell. X-rays X-rays have been in clinical use since their discovery by Roentgen in 1895.
It could typically present helpful information on the presence and web site of different large bowel pathology antibiotic injection for strep buy 150 mg roxithromycin mastercard. Angiography is important if a ruptured intra-abdominal aneurysm is being considered for remedy by the insertion of a stent graft (see Chapter 11) antibiotics for uti otc roxithromycin 150 mg purchase free shipping. When free intraperitoneal fluid is seen antibacterial yoga socks 150 mg roxithromycin discount with amex, it can be precisely sampled utilizing fine needle aspiration and sent for cytological, biochemical or microbiological evaluation. Evidence of pancreatic swelling, haemorrhage or infarction will affirm the prognosis of acute pancreatitis. In truth this is now common for all patients who complain of stomach pain after severe belly trauma. It scans can display intra-abdominal abscesses, unsuspected secondary deposits within the liver, splenic infarcts and splenic trauma. Rectal and low sigmoid tumours may be seen via a inflexible sigmoidoscope and may be biopsied. Flexible sigmoidoscopy and colonoscopy these investi- gations present more data on giant bowel pathology than another checks and may be useful in decompressing the bowel of patients with pseudo-obstruction. Useful data may be obtained about the presence and extent of any colitis, diverticulitis or ischaemic colitis. Management Immediate care Patients with abdominal ache want instant care no matter administration pathway the clinical indicators and the exams described above point out. Patients ought to be relieved of their ache and resuscitated while the history and examination are being performed. Resuscitation with intravenous fluids in patients with a suspected ruptured aneurysm should be administered cautiously as their hypotension is homeostatic and reduces the risk of a deadly rebleed (see Chapter 11). Gentamicin (80 mg bd or tds depending upon blood levels) must be added in cases of extreme Gram-negative peritonitis accompanied by septic shock. Most sufferers being thought-about for operation ought to be aggressively resuscitated in close consultation with the anaesthetist so as to get the patient in the absolute best condition for surgery at a specific time. There is now unequivocal proof that preoperative resuscitation is helpful earlier than emergency surgical procedure, but it should be remembered that over or prolonged resuscitation in the presence of continuing sepsis or blood loss is harmful. It is due to this fact Acute peptic ulceration/gastritis 383 important to formulate a transparent plan of resuscitation and punctiliously monitor the affected person till optimal circumstances are obtained. Continuing fluid and blood substitute within the face of affected person deterioration have to be prevented. Acute ulcers can also develop following a mucosal breach in both the stomach or duodenum. Investigation Clinical diagnostic indicators Acute peptic ulceration causes acute higher abdominal ache, often following consuming, which the affected person typically describes as indigestion. They may have had earlier assaults and be taking non-steroidal antiinflammatory medication. The further investigation and administration of every of these situations is described under. The pain is characteristically episodic (it has a periodicity with exacerbations lasting days or weeks). Patients with duodenal ulcers are inclined to develop pain at night time as the acid ranges rise in the absence of meals to neutralize the acid. There are often no physical indicators associated with uncomplicated peptic ulceration so the primary differential diagnoses may be any of the conditions that cause acute and persistent higher abdominal ache. The main different differential diagnoses are persistent cholecystitis and gall stone colic (see Chapter 18) and the other circumstances listed in Table 17. Tissue biopsy Biopsies must be taken from 4 quadrants of all gastric ulcers to exclude early malignant change. Patients ought to be suggested to keep away from non-steroidal anti-inflammatory medicine if potential and be given assist to give up smoking. A conservative method may be preferable if the patient is in a hostile setting. Blood exams A full blood rely and measurement of the blood urea and electrolytes are advisable earlier than operation however rarely help in confirming the prognosis. Imaging An erect chest radiograph is prone to affirm the clinical diagnosis because it reveals air under the diaphragm in more than 70 per cent of sufferers with a perforated ulcer. Surgical closure is performed via a laparoscope or a laparotomy beneath common anaesthesia. Whereas perforated duodenal ulcers could be closed by easy suture, the perimeters of a perforated gastric ulcer ought to be excised for biopsy before being closed as a end result of some perforated ulcers might be gastric carcinomata. A conservative routine may be employed when the presentation is late or the affected person has different serious medical problems. The pain is usually severe, central and continuous and often radiates to the tip of the scapula. Blood and urine exams A full blood count and liver function exams must be obtained inside 12 hours, especially if the patient is jaundiced. Acute cholecystitis 389 Antibiotics corresponding to a cephalosporin are active against frequent biliary tract organisms and should be given if the affected person is pyrexial or has a marked leucocytosis. Once the prognosis has been confirmed by ultrasound, sufferers may be treated surgically (cholecystectomy) or conservatively. After the establishment of a pneumoperitoneum, a digicam is inserted via a 10-mm port and the fundus of the gall bladder grasped and pulled upwards. Patients who develop repeated acute assaults or those that develop biliary peritonitis, which is usually related to a gangrenous or perforated gall bladder, require urgent surgery. Its investigation and administration is due to this fact much like that described above for acute cholecystitis. The investigations required are the same as these described above for acute cholecystitis, the most important being the ultrasound detection of gall stones. An epigastric mass signifies a phlegmon or a creating pancreatic pseudocyst but it rarely presents in the first 24 hours. Blood checks A serum amylase three or 4 times above regular is almost diagnostic. If the affected person presents late, the urinary amylase should be raised when the blood amylase degree has returned to normal. Haemoglobin, packed cell volume, C-reactive protein and white cell depend should be measured, as should the urea and electrolytes. The patient is usually distressed with signs of shock � tachycardia, tachypnoea � and has cool sweaty peripheries. The stomach indicators could also be generalized and accompanied by distension, and finally a lack of Urine exams the urine ought to be tested, on admission, for bilirubin and urobilinogen. Imaging Plain abdominal X-rays are useful in excluding a perforated ulcer (free gas), gall stones (10 per cent of that are opaque) and a closed-loop obstruction. In the first set of circumstances the baseline investigations and sufficient resuscitation should precede transfer to the operating theatre. Calculation of the severity score Acute pancreatitis must be separated into gentle and severe illness as the administration differs. Evidence of fats necrosis (little white plaques occurring mostly in the omentum and mesentery attributable to the discharge of lipases that digest the fat which then takes up calcium) is diagnostic. Management of gentle pancreatitis Treatment is normally conservative unless the pancreas turns into necrotic � a complication that requires surgical intervention. Monitoring the temperature, pulse, blood stress, Management the administration relies on the clinical indicators and the checks described above. The decisions are: the affected person requires an urgent operation an urgent operation is unquestionably not required urine output and blood sugar ought to be carefully monitored and patients frequently re-examined to detect any change from a mild to a extreme condition. Acute pancreatitis 393 Intravenous fluids must be given particularly if nasogastric aspiration is required to relieve repeated vomiting. Broad-spectrum antibiotics (augmentin, a cephalosporin or metronidazole) are prescribed by most surgeons. After care the presence of gall stones and alcohol consumption Pseudocyst Gastrotomy Cystogastrostomy have to be assessed earlier than discharge from hospital. Counselling may be required to forestall recurrence from alcohol abuse if the cause of the assault was alcohol consumption. Management of severe acute pancreatitis Without skilled resuscitation, sufferers with severe pancreatitis have a mortality fee approaching 50 per cent, so sufferers with severe acute pancreatitis should be admitted to a excessive dependency or an intensive care unit.
In human physiology bacterial gastroenteritis purchase roxithromycin 150 mg mastercard, heme is crucial porphyrin and is bound to proteins to form hemoproteins that include hemoglobin and cytochrome P-450 isoenzymes virus zoo roxithromycin 150 mg buy with visa. Disorders of Purine Metabolism Gout Lesch-Nyhan Syndrome Disorders of Carbohydrate Metabolism Glycogen Storage Disease Type 1a Glycogen Storage Disease Type 1b Disorders of Amino Acid Metabolism Phenylketonuria Homocystinuria Maple Syrup Urine Disease Methylmalonyl-Coenzyme A Mutase Deficiency Key Points the presence of nutritional disturbances or inborn errors of metabolism will significantly affect the administration of anesthesia (Table 15-1) antibiotic generations order 150 mg roxithromycin fast delivery. The pathophysiology and the associated anesthetic implications of probably the most frequently encountered of those ailments are highlighted in this chapter. Inborn errors of metabolism manifest as quite a lot of metabolic defects that may complicate the administration of anesthesia. In some instances, these defects are clinically asymptomatic and manifest only in response to particular triggering occasions, corresponding to ingestion of certain drugs or foods. Enzymes are famous on the suggestions inhibition loop of the sequence, and the sort of porphyria related to the enzyme deficiency is designated on the proper. Enzyme-inducing drugs are the most important triggering components in the development of acute porphyria. Furthermore, being pregnant may be difficult by systemic hypertension and an increased incidence of lowbirth-weight infants. Skeletal muscle weak spot that will progress to quadriparesis and respiratory failure is essentially the most potentially lethal neurologic manifestation of an acute assault of porphyria. Central nervous system involvement with upper motor neuron lesions, cranial nerve palsies, and abnormalities of the cerebellum and basal ganglia are seen less frequently. However, these lesions in combination with autonomic neuropathy and hypovolemia may cause vital cardiovascular instability. However, notwithstanding severe belly pain which will mimic acute appendicitis, acute cholecystitis, or renal colic, medical examination of the stomach usually yields normal findings. Dehydration and electrolyte disturbances involving sodium, potassium, and magnesium could also be distinguished. Tachycardia and hypertension or, less generally, hypotension are manifestations of cardiovascular instability. Complete and prolonged remissions are probably between episodes, and plenty of people with the genetic defect by no means develop signs. It is necessary to notice, nonetheless, that sufferers at recognized risk of porphyria but previously asymptomatic (silent or latent porphyria) might experience their first signs in response to administration of triggering medicine in the course of the perioperative interval. The labeling of drugs as secure or unsafe for patients with porphyria is often based mostly on anecdotal expertise with the utilization of specific agents in porphyric sufferers and reviews of the induction of acute assaults. Alternatively, the motion of medicine on the porphyrin artificial pathway may be investigated in animal fashions. Both cell tradition and animal models tend to overestimate the porphyrinogenicity of medication. It is troublesome to assess the porphyrinogenic potential of anesthetic medication, since different components such as sepsis or stress can also precipitate a porphyric crisis within the perioperative interval. Any classification of anesthetic medication with regard to their capacity to precipitate a porphyric disaster is prone to be imperfect (Table 15-3). Particular care is needed when deciding on drugs for sufferers with acute intermittent porphyria or clinically energetic types of porphyria and when prescribing medicine together, because exacerbation of porphyria is more likely underneath these circumstances. Acute Intermittent Porphyria Of all of the acute porphyrias, acute intermittent porphyria affecting the central and peripheral nervous system produces the most critical signs (systemic hypertension, renal dysfunction) and is the one most probably to be life threatening. The faulty enzyme is porphobilinogen deaminase, and the gene encoding this enzyme is situated on chromosome eleven. Variegate Porphyria Variegate porphyria is characterised by neurotoxicity and cutaneous photosensitivity by which bullous skin eruptions happen on exposure to sunlight as a end result of the conversion of porphyrinogens to porphyrins. The enzyme defect is on the degree of protoporphyrinogen oxidase, and the gene encoding this enzyme is on chromosome 1. Hereditary Coproporphyria Acute attacks of hereditary coproporphyria are less widespread and fewer severe than attacks of acute intermittent porphyria or variegate porphyria. These patients sometimes expertise neurotoxicity and cutaneous hypersensitivity, although these signs are probably to be less extreme than is seen in variegate porphyria. The faulty enzyme is coproporphyrinogen oxidase, encoded by a gene on chromosome 9. Signs and symptoms of porphyria cutanea tarda most often seem as photosensitivity reactions, especially in men older than 35 years of age. Porphyrin accumulation within the liver could be associated with hepatocellular necrosis. Erythropoietic Protoporphyria Erythropoietic protoporphyria is a extra common, however much less debilitating, type of erythropoietic porphyria. Signs and signs embody photosensitivity, vesicular cutaneous eruptions, urticaria, and edema. In occasional sufferers cholelithiasis develops secondary to increased excretion of protoporphyrin. Erythropoietic Uroporphyria Erythropoietic uroporphyria is a uncommon type of porphyria transmitted as an autosomal recessive trait. In the presence of a suggestive household history, willpower of erythrocyte porphobilinogen exercise is essentially the most applicable screening test for sufferers with suspected acute intermittent porphyria. Guidelines for drug choice embody the following: (1) There is evidence that a single publicity to a potent inducer could be nicely tolerated, but not during an acute attack. Note that the American Porphyria Foundation maintains up-to-date data on all aspects of these ailments, and a drug database with details about medication and acute porphyria can be found at. If an acute exacerbation of porphyria is suspected in the course of the perioperative period, specific attention should be given to skeletal muscle strength and cranial nerve function, since these symptoms and indicators might predict impending respiratory failure and an increased risk of pulmonary aspiration. Cardiovascular examination might reveal systemic hypertension and tachycardia, which necessitate treatment earlier than induction of anesthesia. Postoperative mechanical ventilation may be required throughout an acute porphyric crisis. Patients experiencing an acute porphyric crisis have to be assessed carefully for fluid stability and electrolyte standing, particularly the presence of hyponatremia. Preoperative hunger must be minimized, but if a protracted fast is unavoidable, administration of a glucose-saline infusion should be considered, since caloric restriction has been linked to the precipitation of attacks of acute porphyria. Management of Anesthesia Anesthesia has been implicated in triggering acute assaults of porphyria. However, most sufferers with porphyria could be safely anesthetized if acceptable precautions are taken. Patients with evidence of active porphyria or a history of acute porphyric crises are at elevated threat. Short-acting anesthetic medication are presumed to be safe as a outcome of their speedy elimination limits the time of exposure for enzyme induction. However, repeated or prolonged use of these drugs, corresponding to by steady intravenous infusion, may result in a different clinical consequence. It is in all probability going that exposure to several potential enzymeinducing medication may be extra dangerous than publicity to anybody drug, so the anesthetic plan must take this into consideration. Autonomic nervous system blockade induced by the regional anesthetic could unmask cardiovascular instability, especially within the presence of autonomic neuropathy, hypovolemia, or each. Regional anesthesia has been safely used in parturient women with acute intermittent porphyria. Regional anesthesia is used very occasionally, nevertheless, in patients experiencing an attack of acute intermittent porphyria because of concerns about hemodynamic instability, psychological confusion, and porphyria-related neuropathy. Aspiration prophylaxis that features antacids and/or histamine-2 receptor antagonists is acceptable. The availability of relatively short-acting anesthetic medication has likely contributed to the safety of anesthesia in the presence of porphyria. Perioperative monitoring ought to think about the frequent presence of autonomic dysfunction and the chance of blood strain lability. Propofol has been used safely for induction of anesthesia in patients with porphyria, though the use of extended steady infusions of this drug is of unproven security. Ketamine Induction of Anesthesia No particular prophylactic remedy has proven proven profit. All barbiturates should be considered unsafe for anesthetic use even if the porphyria is in a quiescent phase.
They are useful throughout resuscitation and will point out the necessity for oxygen infection resistant legguards purchase roxithromycin 150 mg visa, air flow or a bicarbonate infusion antibiotics kill acne roxithromycin 150 mg cheap with amex. Stool tests Culture and microscopy Stools must be despatched for cul- ture and microscopy in patients suspected of having salmonella bacteria en la sangre discount roxithromycin 150 mg on line, shigella or amoebiasis. Controversy still exists over whether each erect and supine movies of the abdomen should be ordered for all sufferers with undiagnosed belly pain along with an erect chest X-ray. The haematoma related to a ruptured aneurysm could obliterate one of the psoas shadows or be seen as a delicate tissue mass. A chest radiograph can also demonstrate pulmonary consolidation and collapse (conditions which may present with signs much like those of an acute abdomen) and different extra-abdominal causes of the abdominal pain corresponding to fractured ribs (see Chapter 14). A 7-day course of broad-spectrum antibiotics (cephalosporin or metronidazole) should be given in an try to stop the necrotic pancreatic tissue (the phlegmon) becoming infected. A search for rarer causes of acute pancreatitis might be only worthwhile if the condition follows a relapsing course. Myocardial infarction and dissecting aneurysm are an important circumstances to exclude. A barium or gastrograffin swallow will verify the analysis if it reveals contrast medium leaking exterior the wall of the oesophagus. This investigation should be obtained urgently as delay in treatment is the one most necessary factor related to a poor end result. Results the prognosis following a single episode of mild pancreatitis is great with a mortality of lower than 1 per cent, offered precipitating elements such as cholelithiasis and alcohol abuse are treated. By distinction, severe pancreatitis has a mortality rate of around 10 per cent, which rises to 30 per cent if associated with extreme necrosis and practically 40 per cent if necrosectomy is necessary. Investigation Clinical diagnostic indicators this disaster generally follows a suppressed vomit and is adopted by the sudden onset of extreme epigastric pain which may radiate into the lower chest. The presence of subcutaneous emphysema in the cervical region confirms the diagnosis. There are few indications for conservative management if the analysis is made early particularly if the rent in the gastro-oesophageal junction is large. If the prognosis is delayed or the leak small, a pleural drain may be inserted and a conservative approach � fluids, analgesia and antibiotics � continued, however the risks of constant sepsis and deterioration are high with such management. Results the mortality is 10 per cent or less if treated early by surgical procedure, however can rise to 50 per cent if therapy is delayed. It is invariably an organo-axial rotation of the stomach inside a big paraoesophageal hiatus hernia. It usually causes pain in the left hypochondrium that will radiate to the tip of the left shoulder. The primary differential diagnoses are spontaneous splenic rupture and acute pancreatitis within the tail of the pancreas. Investigation Clinical diagnostic indicators Gastric volvulus causes extreme epigastric ache which may radiate up behind the sternum. Management Analgesia and intravenous fluids normally present sufficient aid till the ache subsides spontaneously, however giant spleens with large infarcts might need to be removed by splenectomy. Vomiting is widespread but stomach distension and constipation solely develop at a later stage. Blood and urine exams the urine will be concentrated, the haematocrit excessive and the urea raised with a normal creatinine if the patient is dehydrated. Laparotomy will be the only method to diagnose a number of malignant deposits in the peritoneal cavity and uncommon small bowel tumours. The interval between the pains is short if the obstruction is in the higher jejunum (2�3 minutes) and longer if it is within the lower ileum (15�20 minutes). These two circumstances are the most common causes of small bowel obstruction, so the hernial orifices and belly scars should always be rigorously palpated for irreducible masses. Laparotomy is indicated if the ache is worsening, belly tenderness is developing, the heartbeat rising or the nasogastric aspirate growing in quantity. Foreign our bodies within the ileum similar to a plug of meconium could additionally be milked into the big bowel. A low cardiac output together with massive doses of inotropes given for a quantity of organ failure could cause a patchy ischaemia of both the massive and small gut, as could vasculitis and sickle cell illness. As the ache turns into more extreme, sufferers develop signs of central or general peritonitis (tenderness, guarding, rebound, percussion tenderness and absent bowel sounds). Mesenteric vein thrombosis is often related to a thrombophilia and in addition occurs in girls on the contraceptive pill. The patient can turn into gravely ill by the point the analysis turns into apparent, although the signs and indicators are often delicate. A excessive index of suspicion is required if the analysis is to be made at an early stage. Urgent laparotomy is crucial and should reveal pale or gangrenous bowel with poor peristalsis and the absence of pulsating vessels within the mesenteric arteries. The continuity of the resected bowel may be restored by end-to-end anastomosis or the 2 ends may be brought out on to the skin surface of the abdomen as stomas. This choice is normally based on the appearances of the remaining bowel, with a stoma being preferable if bowel viability is in doubt. Embolectomy catheters may be handed up the divided mesenteric vessels to extract emboli. Bowel continuity may be restored by end-to-end anastomosis at a later stage when the patient has fully recovered. Investigation Clinical diagnostic indicators Obstruction and gangrene of the bowel causes extreme continuous central abdominal pain usually preceded by small bowel colic. Patients lie still with the ache, are normally pale and sweaty and have a tachycardia. The differential prognosis of small bowel strangulation contains the numerous situations listed in Table 17. The urea and electrolytes must be measured if vomiting is a significant symptom, dehydration is suspected or the affected person scheduled for urgent surgery. The vascular compression could additionally be relieved by dividing a band adhesion; gently pulling the bowel out from the constricting neck of the hernial pouch; or by untwisting a volvulus. Signs of peritonitis, tenderness, guarding and rebound tenderness develop over a variable period. Eventually, if left untreated, the entire stomach turns into distended, rigid and silent, and the affected person develops indicators of toxaemia and shock. Blood tests A full blood count is more likely to present a leucocytosis, and a raised haematocrit. Results the results of the above therapy are normally good until the analysis is missed and remedy is delayed. The mortality price rises above 5 per cent if the affected person is old or infirm and if the resection of lifeless bowel is delayed beyond 24 hours of its onset. Short gut syndrome can occur if an entire volvulus has to be resected and this carries significant morbidity and mortality. Complications Intraperitoneal abscess,wound infection, atelectasis and multi-organ failure are frequent. Although half of the patients are cured by an enema many nonetheless require cautious fluid substitute over the following few days. Results the mortality varies between 5 per cent and 10 per cent, relying on the age and fitness of the patient, the cause of the perforation and the time frame that has lapsed between the onset of the perforation and the onset of therapy. Ruptured abdominal aortic aneurysm 403 Surgery When surgery has to be carried out, an enterostomy is made within the proximal ileum and saline is irrigated distally to wash out the meconium plugs. Treatment is usually by gastrograffin enemas, but sometimes surgery is required and enterotomies could additionally be essential to clear out the inspissated lots. Other tumours of the small bowel corresponding to adenoma, lipoma, sarcoma and secondary deposits are very rare. Investigation Clinical diagnostic indicators Most small bowel tumours current with subacute obstruction or gastrointestinal haemorrhage. Management this is conservative until the diagnosis is doubtful or the signs turn into very extreme, when surgical resection and anastomosis to healthy bowel might avoid the chance of dehiscence. Management Surgical resection of the small bowel and its mesentery to clear the lymph nodes is the only effective therapy. Chemotherapy is indicated in patients with a lymphoma or in those who develop the carcinoid syndrome.

Because obese girls have a better likelihood of requiring cesarean supply and the danger of general anesthesia is substantial on this affected person inhabitants antibiotic prophylaxis for joint replacement buy 150 mg roxithromycin fast delivery, early epidural analgesia presents another advantage-the capability to prolong the block for surgical anesthesia antimicrobial essential oils discount 150 mg roxithromycin with visa. Long needles may be required to attain the epidural house and ought to be available within the labor and delivery unit infection years after root canal purchase 150 mg roxithromycin with mastercard. Placement of the affected person within the sitting, rather than the lateral, position ought to facilitate successful identification of the epidural space. Because the failure rate for epidural analgesia is increased in obese sufferers, these sufferers must be monitored regularly Labor Analgesia Advanced Maternal Age In 2002, approximately 14% of all births within the United States had been to women 35 years or older. In Canada in 2002, 30% of all births had been to ladies 30 to 34 years of age, and 14% have been to women 35 to 39 years of age. In 2008, births to girls older than 40 years made up 3% of births within the United States, triple the speed of twenty years earlier. Patients and health care professionals believe that advanced maternal age leads to poor outcomes. The rationale for this view is the upper incidence of continual medical conditions in older patients. Indeed, superior maternal age is independently associated with maternal morbidities, together with gestational diabetes, preeclampsia, abruptio placentae, and cesarean delivery. Healthy women of superior maternal age can be expected to have uneventful pregnancies and deliveries. However, nearly half of sufferers of superior maternal age have preexisting medical conditions or develop pregnancy-related sickness. Multiple gestations are extra common in older pregnant girls, as are miscarriage, preterm delivery, and fetal complications corresponding to congenital anomalies, low birth weight, and intrauterine and neonatal death. Fetal alcohol syndrome occurs in approximately one third of infants born to mothers who drink greater than 3 oz of alcohol per day during being pregnant. However, studies have reported neurobehavioral deficit, intrauterine growth retardation, and different congenital abnormalities in infants of average alcohol shoppers. Management of anesthesia in pregnant sufferers who abuse alcohol entails the identical concerns as anesthetic care of nonpregnant alcohol abusers (see Chapter 25). Prenatal care ought to consider early analysis of pregnancy-related illnesses to enable early and aggressive administration of these problems. However, superior maternal age can be independently related to an elevated probability of cesarean supply, and charges of patientrequested cesarean delivery are much higher in women older than 34 years of age than in ladies 25 years of age or youthful. Because pregnant smokers are comparatively young, often there are minimal indicators and signs associated with tobacco abuse in this population. A robust association is found between cigarette smoking and low toddler delivery fee, abruptio placentae, and impaired respiratory perform in newborns. In those who smoke more than 20 cigarettes per day, the incidence of premature supply doubles. Sudden toddler demise syndrome happens far more regularly in infants of moms who smoke. As with alcohol abuse, the anesthetic considerations for care of tobacco-abusing parturient sufferers are just like those for care of nonpregnant patients who smoke. Many commonly abused substances are mind altering or affect the cardiovascular system when the affected person is in an acutely poisonous state. Substances abused in pregnancy parallel these abused in society at massive: alcohol, tobacco, opioids, and cocaine are frequently abused. These embrace infectious complications similar to human immunodeficiency virus an infection and hepatitis. Patients could develop local abscesses or, extra considerably, may have endocarditis or thrombophlebitis. A pregnant affected person admitted while receiving long-term opioid therapy must be maintained on that therapy throughout her being pregnant and into the postpartum interval. In reality, withdrawal from opioids during the third trimester can end result in perinatal asphyxia or dying of the neonate. Withdrawal of the neonate from opioids can present as respiratory distress, seizures, hyperthermia, and sudden infant dying syndrome. Considerations for the anesthetic care of opioid-dependent parturient ladies are similar to those for nonpregnant opioid-dependent patients. Management of Anesthesia Approximately 4% of pregnant ladies are heavy alcohol customers. Cocaine is related to maternal cardiovascular problems similar to systemic hypertension, myocardial ischemia and infarction, cardiac dysrhythmias, and sudden demise. Sudden will increase in systemic blood stress may be the main cause of cerebral hemorrhage. Subarachnoid hemorrhage, intracerebral bleeding, aneurysmal rupture, and seizures have been associated with cocaine use throughout pregnancy. Thrombocytopenia might occur following cocaine use and end in extended bleeding occasions. The maternal use of cocaine may result in metabolic and endocrine modifications in both the fetus and the mother, which presumably displays cocaineinduced release of catecholamines. Pulmonary problems (asthma, chronic cough, dyspnea, pulmonary edema) happen most frequently in parturient women who smoke free-base cocaine. An increased incidence of great obstetric issues is seen in parturient ladies who abuse cocaine during being pregnant (Table 26-12). The incidence of spontaneous abortion, stillbirth, and preterm labor is increased. High spontaneous abortion charges could additionally be associated to cocaine-induced vasoconstriction, enhanced uterine contractions, and abrupt adjustments in systemic blood stress. Identification of parturient ladies abusing cocaine is troublesome, as a outcome of urine checks detect metabolites of cocaine for only 14 to 60 hours after use. One of the only most important predictors of cocaine abuse is the absence of prenatal care. Cocaine use in the course of the third trimester could end in immediate uterine contractions, elevated fetal exercise, abruptio placentae, and preterm labor. Uteroplacental insufficiency ends in fetal intrauterine growth retardation, microcephaly, prematurity, and decreased birth weight. Maternal systemic hypertension and vasoconstriction could also be the purpose for the increased incidence of abruptio placentae in cocaineabusing parturient girls. Cocaine effects on the fetus may manifest as an increased incidence of meconium staining and low Apgar rating at birth. Evaluation of parturient patients suspected of cocaine abuse consists of electrocardiography and presumably echocardiography to check for the presence of valvular heart disease. Cocaine-induced thrombocytopenia have to be excluded if regional anesthesia is planned. Epidural Management of Anesthesia Prognosis Diagnosis Obstetric complications associated with cocaine abuse during being pregnant Spontaneous abortion Preterm labor Premature rupture of membranes Abruptio placentae Precipitous delivery Stillbirth Maternal hypertension Meconium aspiration Low Apgar scores at start anesthesia is instituted progressively, with attention to hydration and left uterine displacement to forestall hypotension. Hypotension caused by rapid-sequence induction of general anesthesia or establishment of regional anesthesia usually responds to ephedrine, though long-term cocaine abuse can deplete catecholamines and theoretically blunt responses to indirectacting vasopressors. Thus, phenylephrine could be the better option for treatment of hypotension in these patients. Esterbased native anesthetics, which bear metabolism by plasma cholinesterase, may compete with cocaine, so that metabolism could additionally be decreased for each medication. Body temperature increases and sympathomimetic effects associated with cocaine could mimic malignant hyperthermia. The fundamental precept of electronic fetal monitoring is to correlate adjustments in fetal heart rate with fetal well-being and uterine contractions. In 2009 the American College of Obstetricians and Gynecologists revealed a revised apply bulletin updating the nomenclature for intrapartum fetal monitoring. A threetier interpretation system was established that combines the assessment of baseline rate, beat-to-beat variability, accelerations, and periodic decelerations. Conversely, fetal distress ensuing from arterial hypoxemia, acidosis, or central nervous system harm is related to minimal to absent beat-to-beat variability. Drugs administered to parturient patients may blunt or eliminate fetal heart fee variability, even within the absence of fetal misery. Drugs most frequently related to loss of beatto-beat variability are benzodiazepines, opioids, barbiturates, anticholinergics, and native anesthetics, as used for continuous lumbar epidural analgesia. In addition, lack of heart rate variability may be current normally in the premature fetus and during fetal sleep cycles. When beat-to-beat variability persists regardless of late decelerations, the fetus is still more likely to be born vigorous.






