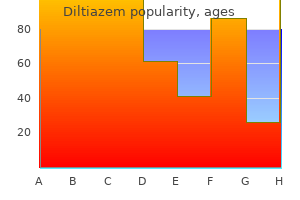
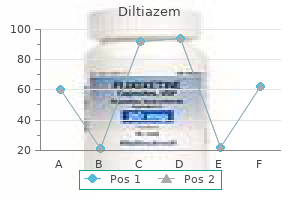
Diltiazem
Diltiazem
Diltiazem dosages: 180 mg, 60 mg
Diltiazem packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Knee dislocations are necessary as a end result of they produce intensive disruption of the ligaments that stabilize the knee and the encircling soft tissue buildings medications you can crush order diltiazem 60 mg with amex, including the popliteal artery medications neuropathy generic 60 mg diltiazem with amex. Complete disruption of one or both of the collateral ligaments is anticipated with this extreme damage medicine 5000 increase cheap diltiazem 180 mg mastercard. Frequently, the sample of bone contusions permits definition of the kind of knee dislocation. This is a vital statement as a end result of posterior and posterolateral dislocations have a excessive association with peroneal nerve harm. Magnetic Resonance Imaging A knee dislocation is classified in accordance with the place of the tibia relative to the femur. There are five several varieties of dislocations: (i) anterior, (ii) posterior, (iii) lateral, (iv) medial, and (v) posterolateral. Segond Fracture the Segond fracture, or avulsion of the anterolateral facet of the lateral tibial plateau, is a radiographic entity that signifies underlying trauma to the anterolateral nook structures of the knee. This harm is seen most frequently in individuals who take part in long-distance running and cycling. The layered configuration of the quadriceps tendon enables discrimination between partial and full tears. Discontinuity of any of the tendinous layers is consistent with partial tears typically involving the rectus femoris element. Transection of all the layers is diagnostic of a complete rupture and could additionally be related to a mass of edematous tissue and hemorrhage seen as excessive sign on T2W pictures. The patellar tendon additionally has homogeneous low signal depth look except for small occasional triangular areas of intermediate sign depth immediately below the patella and adjoining to the tibial tuberosity. A giant collection of adipose tissue, the infrapatellar fat pad of Hoffa, rests just posterior to the patellar tendon. In symptomatic sufferers, the findings could additionally be accompanied by patellar monitoring disorders in as many as 45% of patients. Acute Patellar Tendon Disruption A minority of patellar ligament accidents are full tendon disruption resulting from acute macrotrauma in the setting of sports-related exercise. Femoral Trochlear Groove the femoral trochlear groove offers a mechanical restraint that helps stabilize and function a guide for the patella as it articulates with the groove during joint function. In the axial airplane the posterior apex of a normal patella is centered instantly above the intercondylar femoral sulcus. Shallow sulcus angles (larger sulcus angle measurements) predispose to patellar instability. Affected sufferers are both athletes and nonathletes who experience chronic anterior knee ache that localizes to the inferior patellar pole on physical examination. Most patient show patellar alignment abnormality, similar to patella alta or lateral subluxation. Patients usually respond properly to conservative treatment, which usually entails taping the superior pole of the patella. The avulsed free finish of the retinaculum is commonly frayed and thickened and fluid might dissect around a muscular slip of the vastus medialis muscle. A low using patella (patella baja or profunda) happens in quadriceps tendon rupture however can be found with paralytic neuromuscular problems, achondroplasia and juvenile rheumatoid arthritis. Patellar shape: Wiberg has proposed a three half classification to embody the majority of patellar aspect configurations. This process must be repeated at three completely different section locations in order that the whole excursion of the patella could be evaluated because it articulates with the femoral trochlear groove. Compared with the incremental, passive positioning approach, a more physiological examination is obtained and in sure cases abnormal patellar tracking is more obvious throughout lively movement. Motion Triggered Cine Technique In this system, a particular nonferromagnetic device incorporates a trigger system that senses the movement of the patella. The patient is placed supine on the positioning gadget and a single patellofemoral joint is flexed and prolonged repeatedly whereas gradient echo photographs are obtained utilizing a circular floor coil. Articular cartilage perform is misplaced with harm to chondrocytes, collagen or proteoglycans. With more severe damage cracks, fissures, and focal defects form in the cartilage. Because of its hydropic composition regular hyaline cartilage demonstrates intermediate signal depth on T1-weighted pictures compared with the low signal intensity of the cortex and fibrocartilaginous menisci. On typical T2-weighted images also hyaline cartilage displays an intermediate sign depth. In the presence of joint effusion T2-weighted images create an arthrogram like impact with hyperintense synovial fluid improving the delineation of thinner cartilage surfaces. There is poor contrast; nonetheless, between articular cartilage and subchondral bone on typical T2-weighted pictures and in the absence of joint effusion, surface or contour irregularities is probably not resolved. This sequence can also be helpful in demonstrating early adjustments of subchondral bone in areas of overlying articular cartilage injury. Gradient echo imaging is helpful with respect to imaging geometry, speed and contrast. Three-dimensional imaging considerably improves sign to noise ratios at excessive spatial decision. With gradient echo strategies articular cartilage demonstrates high sign intensity. However, articular cartilage and articular fluid show similar excessive signal intensity, and important cartilaginous accidents could also be missed using gradient echo techniques if joint fluid and articular cartilage are isointense. This methodology permits identification of abnormalities that is probably not noticed during unloaded examination. By deforming underneath strain the articular cartilage tremendously will increase the efficient contact area between femoral condyles and tibial plateaus, significantly decreasing the pressure transmitted across these joints. The cartilaginous matrix of articular cartilage permits the knee to withstand giant native pressures, as much as 5 instances normal pressures. Articular Cartilage Structure and Damage Articular cartilage is composed of an extracellular matrix maintained by a relatively small inhabitants of chondrocytes. All three imaging planes are helpful; however, the sagittal aircraft is the best single aircraft for analysis of articular cartilage as a end result of it provides close to orthogonal images of a lot of the articular cartilage surfaces within the knee. The quantitative findings have a very essential role in evaluating early osteoarthritis at a stage when the changes are doubtlessly nonetheless reversible. They are a consequence of traumatic bone necrosis following impact of two opposing articular surfaces. Only contrast-enhanced images can differentiate between synovium and joint effusion. Subchondral bone attrition: Subchondral bone attrition is outlined as a despair or flattening of the subchondral bony floor unrelated to gross fracture. Popliteal cysts might arise from any situation that causes a rise in synovial fluid inside the joint and are regularly seen in association with tears of the posterior horn of the medial meniscus. In contrast to popliteal cysts, ganglion cysts are viscous synovium stuffed plenty with mucopolysaccharide rich contents. Other bursites like prepatellar bursites and pes anserine bursites may be seen. A T1-weighted picture in at least one plane ought to be included within the study to enhance the identification of unfastened our bodies that contain marrow fat. The exclusive use of fat suppressed sequences may lead to the loose bodies being missed. Pannus tissue is seen as an space of increased sign depth on these contrast enhanced photographs adjacent to the low sign intensity joint fluid. Marginal and subchondral erosions with diffuse loss of hyaline articular cartilage are evident on both medial and lateral femoral articular surfaces. Hypertrophied synovial lots stay comparatively low in signal depth on T1 and T2W pictures. This irregular infrapatellar fat pad sign is seen in patients with rheumatoid arthritis, pigmented villonodular synovitis Tuberculosis of the Knee Magnetic resonance imaging is superb for detecting early adjustments of tuberculosis. Histologically, the lesions current with fibrous synovial proliferation, infiltration by histiocytes, multinucleated large cells and hemosiderin laden macrophages and hemosiderin staining of the synovium presumably from recurrent hemorrhage. These cartilaginous islands may turn into dislodged producing both calcified and noncalcified free our bodies. The arthropathy consists of musculoskeletal stiffness, joint pain and joint effusion. Synovial thickening and enhancement, synovial bands and effusions have been described.
Diseases
Understanding primary features of liver hemodynamics is necessary to analyze diagnostic pictures symptoms lead poisoning diltiazem 60 mg cheap. These are: 1418 Section 3 Gastrointestinal and Hepatobiliary Imaging Bridging Collaterals (Hepatopedal) In extrahepatic obstruction of the portal venous system bridging collaterals assist restore hepatopedal move medicine 20th century effective diltiazem 180 mg. Patients commonly current with a self-palpable mass (the enlarged spleen) quite than variceal bleed treatment xanthelasma eyelid discount 60 mg diltiazem otc. A female dominance, male dominance or no sex prediliction has been reported by numerous investigators. It is characterized by well-tolerated episodes of gastrooesophageal variceal hemorrhage in a young affected person with prominent splenomegaly. The primary lesion is an obliterative portovenopathy of the liver with patchy segmental, subendothelial thickening of intrahepatic portal venous radicles with variable obliteration or recanalization and scarring and fibrosis resulting in presinusoidal irregular blood flow. Fibrosis and nodule Table 1: Etiology and classification of portal hypertension6 i. Presinusoidal: Noncirrhotic portal fibrosis, hepatic schistosomiasis, congenital hepatic fibrosis, sarcoidosis and lymphoma 2 Postsinusoidal hepatic cirrhosis (alcoholic, postnecrotic) and veno-occlusive illness B. Chest X-ray could show a dilated azygos system while X-ray stomach might present nonspecific findings of hepatosplenomegaly and haze due to ascites. Gastric duodenal and rectal varices can be detected utilizing barium contrast research nevertheless, their role has become restricted with the widespread use of endoscopy. Doppler evaluation could also be limited by weight problems, ascites and interference by bowel gasoline. Computed Tomographic Imaging Computed tomography can reveal the portal venous system and portosystemic collaterals in any a part of the body with minimal interference from gasoline, bone or fat not like sonography. The scan protocol consists of an initial noncontrast examine to establish the liver location and volume of interest. Subsequently 100�120 mL of contrast medium is run via a stress injector at the fee of 3�3. Arterial part images are initiated 25�30 sec after initiation of distinction material. Portal venous section pictures are acquired after a delay of 60 sec after initiation of distinction and an extra acquisition could also be made at a hundred and eighty sec for hepatic venous part pictures. Patient may be given 750 mL of water orally before the scan as it permits visualization of even small varices in the gastric wall. Furthermore it was unimaginable to get hold of pure arterial part or venous part images. The acquisition volume ought to embody the entire portal and mesenteric venous system. In addition the absence of nephrotoxic contrast media and lack of ionizing radiation make it a beautiful imaging modality. On gradient echo pulse sequences flowing blood is brilliant whereas thrombus is hypointense. Blurring: Breathholding twice in a row to seize each the arterial and venous section is troublesome for many patients. There is marked dilatation of the portal vein (19 mm) with selective dilatation of the left department. Portal Vein, Superior Mesenteric Vein and Splenic Vein Diameter the traditional portal vein diameter is 9�12 mm in quiet respiration. In normal individuals, the diameter of these veins will increase by 20�100% from quiet to deep inspiration. Helical move is present in some regular people and may simulate reverse or bidirectional circulate. The fasting mean flow velocity is approximately 12�18 cm/sec (range 12�23 cm/sec) and has respiratory cycle variation reducing on inspiration and growing on onset of expiration. Portal vein diameter is done at the heart of the portal vein at a recognized angle of insonation lower than 60�. Mean velocity should be calculated over tracing 4�6 sec lengthy to be able to keep away from fluctuation in move velocity. Flow reversal must be assessed all through the portal venous system as reversal could also be segmental. The essential collaterals as follows: z Left gastric (coronary vein)-Diameter of the normal coronary vein is lower than four mm, whereas a diameter greater than 7 mm is proof of portosystemic stress gradient exceeding 10 mm Hg. However, the chance of hepatic encephalopathy is elevated Occasionally, collaterals could also be seen throughout the gallbladder wall and these are often distinguished in extrahepatic portal obstruction. Other collaterals which have been described include splenoretroperitoneal, splenocaval, omphaloiliocaval and splenoportal. Flow patterns in the hepatic veins rely upon each cardiac physiology and liver histology. Altered hepatic vein waveforms are seen in no much less than 50% of patients with cirrhosis with flattening of the phasic oscillations. Hepatic artery diastolic velocity normally is less than the height portal vein velocity of about 18 cm/sec. If the Doppler study reveals hepatic arterial diastolic velocities larger than the portal vein, one ought to suspect parenchymal illness in the liver. The congestion index is the ratio between the cross-sectional space and the mean move velocity of the portal trunk. Measurement of the diameter and size of the principle portal vein may be performed on 2D multiplanar reconstructions and axial photographs. Direct sagittal photographs are useful within the evaluation of paraumbilical veins and coronal images are useful for mesenteric and splenorenal varices. A single 5�10 mm thick 2D phase distinction picture is acquired in an indirect airplane perpendicular to the portal vein. On the 2D section contrast images, background tissues are gray whereas circulate perpendicular to the image airplane is shiny in a single direction and black within the other. This allows quick visualization of fluid movement thereby enabling calculation of flow velocity from fluid motion. Extrahepatic Portal Hypertension: Prehepatic Portal Vein Occlusion Portal vein occlusion may be brought on by thrombosis, tumor invasion or compression. There are several patterns of portal vein occlusion together with major stem embolization, branch embolization, cast-like embolization and partial obstruction. Thrombosis may be precipitated by stagnant portal flow in patients with cirrhosis. Other causes embrace infections, corresponding to neonatal/umbilical sepsis, intraperitoneal inflammatory processes, corresponding to pancreatitis and appendicitis hypercoagulable states and surgical procedure. Malignancy may lead to portal vein thrombosis due to a hypercoagulable state or postradiotherapy. The most typical etiologic issue for portal vein thrombosis in children was discovered to be infection (approx. On colour Doppler examination, colour fill may be absent in an occluded section or a trickle of flow could also be seen across the thrombus. The occluding thrombus frequently dilates the main portal vein and its branches noticeably. Cavernous transformation is the principle manifestation of persistent portal vein thrombosis producing a tangle of tortuous vessels within the porta hepatis. Partial transsplenic shunting of venous blood due to flow reversal within intrasplenic tributaries of splenic vein draining to perisplenic floor collaterals has been reported in sufferers with portal cavernoma and also in cirrhosis. Other features are a transient attenuation distinction, segmental staining and retrograde portal department filling, because of a relative increase in hepatic arterial flow which compensates for the lower in portal blood flow. These are seen on the porta and within the area of portal confluence where they could be mistaken for a pancreatic mass on unenhanced or nondynamic scans. The commonest causes of splenic vein occlusion are pancreatitis and pancreatic carcinoma. Other less frequent causes include idiopathic thrombosis, retroperitoneal hematoma or tumor and hematological problems. The explanation for the fistula could also be traumatic, congenital, atherosclerotic or idiopathic. These shunts decompress the gastroesophageal varices while sustaining hepatopedal move in the mesoportal venous bed to have the ability to scale back incidence of hepatic encephalopathy.
Also called a horizontal cleavage tear this is the most common kind of tear to be associated with a meniscal cyst medications xarelto 60 mg diltiazem cheap otc. These vary from a small harm alongside its free edge to a large tear extending via its entire circumference symptoms 8 weeks safe 180 mg diltiazem. Magnetic resonance photographs obtained perpendicular to the orientation of a radial tear demonstrate the tear as a small hole or cleft within the meniscus (cleft sign) which can sometimes be noticed to transfer across the meniscus on successive pictures (marching cleft sign) symptoms 7dpiui discount 60 mg diltiazem mastercard. A partial thickness radial tear will demonstrate blunting or abrupt truncation of the apex of the meniscus (truncated triangle sign). A full thickness radial tear severely compromises meniscal perform by disrupting the important circumferential collagen bundles such that the meniscus can not develop the "hoop stresses" necessary to disperse an axial load. Root tears: Root tears are full thickness radial tears on the central tibial attachments of the menisci. Radial tears should be suspected in instances of peripheral subluxation of the concerned meniscus. Chapter 194 Magnetic Resonance Imaging of the Knee 3175 Longitudinal Tears Vertical longitudinal tears make up the common bucket deal with tear that happens in about 10% of meniscal tears. The regular meniscus has a physique width of about 9 mm, which is seen on sagittal pictures as a single slab of meniscal tissue that has a form much like a bow-tie. When the inner edge of the meniscus displaces, a bucket handle tear is well diagnosed by noting only one instead of the conventional two physique segments current on the outermost sagittal images through the meniscus. This known as the "absent bow-tie sign"10 and could be the solely indication of a bucket handle tear. Normally, there are only two buildings in the intercondylar fossa, the anterior and the posterior cruciate ligament. Any different construction within the intercondylar fossa is irregular and a displaced meniscal fragment is the most probably possibility. The displaced fragment may flip over the anterior horn of the affected meniscus which is called an "anterior flipped meniscus signal". A new sign has been described lately for the diagnosis of bucket handle tears referred to as the "V signal". The V sign is seen on the axial images and is seen on the junction of the displaced fragment and the meniscus, which is in place. The V sign, when seen on axial photographs, is extremely suggestive of a bucket deal with tear. Except for the peripheral 10�25% of the meniscus which is equipped by the perimeniscal capillary plexus the meniscus in adults is relatively avascular. Because of the wealthy vascularity in peripheral portion of the meniscus (red zone), this type of tear is more likely to heal with conservative therapy or operative restore, whereas tears confined to the inside white zone of the meniscus (avascular) should be debrided or resected. It can even occur alongside the posterolateral nook of the joint the place the lateral meniscus is attached by the popliteal meniscal fascicles. This harm is identified when true fluid sign depth is seen interposed between the meniscus and adjoining capsule or when the popliteal meniscal fascicles are disrupted. Popliteus Tendon There is usually a minimal of a small amount of fluid throughout the popliteus tendon sheath that could be mistaken for a tear at the junction of the posterior horn and physique of the lateral meniscus on sagittal or coronal scans. The posterior horn of the lateral meniscus courses slightly upwards because it extends into the posterior intercondylar notch. This is due to the magic angle phenomenon caused by fifty five degree orientation of this meniscus with respect to the static magnetic area. Pulsation Artifact from the Popliteal Artery Phase artifacts propagating from the popliteal artery could mimic a tear within the posterior horn of the lateral meniscus on sagittal scans. [newline]Misdiagnosis could be avoided by recognizing the alternating strains of increased and decreased sign propagating across the whole picture at that degree. Surgical Considerations in Meniscal Tear Meniscofemoral Ligaments Similarly, the attachment of the meniscofemoral ligaments of Humphrey or Wrisberg to the posterior horn of the lateral meniscus could additionally be mistaken for a tear on sagittal scans. Again, examination of sequential sagittal or applicable coronal scans ought to enable for correct analysis. The paramount aim is to protect as much meniscal tissue as potential to lessen the likelihood of developing osteoarthritis. Tear Location the most important think about predicting the success of a meniscal restore is the place the tear is situated within the meniscus. It is also essential to describe any meniscal tissue that has turn into displaced into a para-articular "gutter" so that the arthroscopist is prepared to probe for and resect the fragment, which might in any other case be missed. There are several mechanisms of harm associated with ligament and tendon disruptions, a knowledge of which enables the radiologist to analyze systematically the buildings of the knee affected and maximize the detection of pathology. Small partial tears (involving lower than half the peak of the meniscus) and radial tears measuring less than 5 mm in size even have a higher price of therapeutic than do larger tears. Most horizontal tears are additionally not amenable to restore and the surgeon usually resects either the superior or inferior flap, leaving the opposite in situ. It usually has a striated look with some high sign within it particularly at its insertion on the tibia. An irregular or wavy contour and disruption of fibers also suggests a whole tear. In partial tear, although the bulk of the ligament seems to be intact with a relatively normal axis, there may be localized angulation of the ligament at the website of fiber disruption. False-negative analysis might result from the formation of scar tissue with adherence of anterior cruciate ligament to the publish cruciate ligament simulating a traditional course and sign of the anterior cruciate ligament. The invested deep fascia of the sartorius muscle, which overlies the gastrocnemius muscle, forms probably the most superficial layer. The tibial collateral ligament, the first support construction, extends from the medial epicondylar region of the femur to the medial surface of the proximal tibia and spans about 8�9 cm in size. Magnetic Resonance Imaging Posteromedial nook accidents often end result from a valgus stress mixed with rotational forces. It has a fusiform configuration and seems uniformly hypointense on all imaging sequences. A focus of marrow edema may be current when the posterior indirect ligament avulses. The arcuate ligament is as Y-shaped construction that represents thickening of the posterolateral joint capsule. These are seen as low signal intensity buildings on all pulse sequences and almost uniform in thickness. Contour modifications, corresponding to thickening and irregularity, are extra typical of subacute or old accidents. Most full ruptures contain the conjoined tendon and will produce a small avulsion of the styloid strategy of the fibular head. Complete tears of the popliteal tendon trigger enlargement of the muscle belly and the retracted tendon terminates abruptly. Isolated popliteal injuries are uncommon, as a outcome of most are associated with concomitant injuries of the arcuate ligament complicated. The tendons of the gastrocnemius muscle tissue together with the soleus tendon form the Achilles tendon, which inserts on the posterior tubercle of the calcaneus. The major action of the gastrocnemius muscle is plantar flexion of the foot but in addition serves as a passive supportive construction of the posterior joint capsule. The gastrocnemius muscle arises as two heads from the posterior floor of Magnetic Resonance Imaging Gastrocnemius accidents mostly are brought on by hyperextension of the knee or when the tibia posteriorly dislocates throughout knee flexion. Magnetic resonance imaging can assess the chronicity of the hematoma by the overall appearance of the merchandise of hemoglobin degradation. A full rupture of the gastrocnemius head is associated with retraction of the muscle belly. Bone marrow usually demonstrates a similar response whatever the insult, i. A systematic method of analyzing the sample of the marrow pathology and associated abnormalities helps in arriving at a particular diagnosis. A minority <5% fail to resolve by 3 months probably secondary to repetitively utilized trauma. A technique of grading severity of marrow edema particularly trauma induced marrow edema relies on diffusion imaging. Trabecular disruption results in increased multidirectional movement of water; therefore, a recorded change in marrow diffusion is an objective marker of the severity of marrow injury. A excessive recorded diffusion coefficient can be utilized as on early indicator of severe marrow harm and can be optimally managed by a nonweight-bearing regimen.
Surface osteosarcoma � Periosteal(chondroblastic) � High-gradeperiosteal � Juxtacortical(parosteal) c symptoms 9dpo discount diltiazem 60 mg without a prescription. A chondroblastic variety of osteosarcoma may happen when a large part of the tumor is composed of cartilage medicine used during the civil war diltiazem 60 mg purchase with mastercard. Although the prognosis for this sort of osteosarcoma is poor as in comparability with medicine bow wyoming diltiazem 180 mg generic online conventional osteosarcoma, effective chemotherapy has improved survival. Small cell osteosarcoma17 (approximately 1%) is similar to typical osteosarcomas in its clinical presentation and radiographic look. The radiographic options range from predominantly osteolytic or ground glass to predominantly sclerotic. The tumor might show geographic destruction and is regularly expansile with common cortical destruction and solid periosteal response. Due to its relatively benign look, the tumor could additionally be mistaken for fibrous dysplasia, osteoblastoma or a low-grade chondroid tumor. Intracortical osteosarcomas are the rarest form of osteosarcoma, accounting for lower than 1% of cases. The tumor appears as a small lytic lesion surrounded by thickened cortex, resembling an osteoid osteoma or osteoblastoma. These tumors have a greater prognosis than the standard intramedullary osteosarcoma. The primary differential diagnoses of osteosarcoma in its early phases are osteomyelitis and trauma. Once the plain radiograph reveals a medullary lesion, the prognosis usually lies between osteosarcomas and different malignancies, including metastasis. Of the benign lesions, osteoblastoma, giant cell tumor, osteoid osteoma and osteomyelitis, notably the sclerosing variety of Garr� has to be thought of. The metastases are often subpleural in location and generally associated with a pneumothorax. The prognosis of osteosarcoma has improved greatly with using chemotherapy and limb-preserving surgery. Presently the treatment requires multiple cycles of chemotherapy earlier than surgical resection. Periosteal Osteosarcoma20 Periosteal osteosarcoma is an intermediate grade chondroblastic osteosarcoma accounting for 1�2% of all osteosarcomas. The age distribution, gender and presenting options are much like conventional osteosarcomas. This entity is characteristically diaphyseal in location and the center of the tumor is situated on the surface of the bone with a saucerlike shallow area of adjoining cortical bone destruction. Magnetic resonance imaging classically exhibits hyperintensity on T2W photographs as a outcome of the chondroblastic nature of the lesion. Juxtacortical/Parosteal Osteosarcoma this uncommon tumor is hooked up to the floor of the affected bone and has a tendency to encircle it. Lateral radiograph of the knee exhibits a dense, lobulated mass arising from the posterior distal femur. This is the classical location for parosteal osteocarcoma; (B) Paraosteal Osteosarcoma. This tumor is kind of solely present in long bones, with 70% occurring across the knee specially the posterior aspect of femur. Magnetic resonance imaging exhibits a low signal equal to regular cortex within the poorly cellular ossified component with a variable increase in signal intensity from the peripheral more lively factor of the tumor. The differential prognosis includes a closely mineralized osteochondroma and juxtacortical myositis ossificans, which is differentiated by its peripheral mineralization pattern. High-grade Surface Osteosarcoma this could be a very uncommon lesion arising from the floor of the bone but having the identical histological features as conventional central osteosarcomas. The most typical website is the gentle tissues of the thigh, but they may also be discovered within the pleura, dura of brain, coronary heart valves, retroperitoneum, axilla, breast, and so forth. These uncommon tumors Chapter 193 Malignant Bone Tumors 3149 present the identical histological pattern as different osteosarcomas. Mineralization of the matrix can suggest the diagnosis but differentiation from different gentle tissue sarcomas which calcify. Spinal involvement might happen, presenting as an irregular, nodular radiopaque mass or ivory vertebra. The comparable measurement of all the lesions with absence of lung metastases differentiates this disease from metastatic osteosarcoma. However, lung metastases do seem later in the middle of the illness and the illness is invariably fatal. Rarely osteosarcoma develops in association with osteonecrosis, fibrous dysplasia, osteogenesis imperfecta, metallic prosthesis and continual osteomyelitis. There can also be associated features of radiation changes in the underlying bone within the type of radiation osteitis and marrow infarction. It arises from chondroblasts and collagenoblasts, thus producing solely cartilage and collagen. It is the third most typical main malignant tumor of bone after multiple myeloma and osteosarcoma, accounting for about 10% of all major bone tumors. It normally develops later in life than osteosarcoma and carries a significantly better prognosis as a end result of metastases typically happen late. Chondrosarcoma can be divided into two broad categories that are: main and secondary. A main chondrosarcoma is believed to be malignant from the outset while a secondary chondrosarcoma arises in a pre-existing bony lesion, normally an enchondroma or an osteochondroma and rarely in chondromyxoid fibroma or chondroblastoma. A chondrosarcoma can also be classified according to its histological grade as low grade (grade 1: 45�50% of cases), myxoid (grade 2: 30�40% of cases), high grade (grade three: 8�25% of cases) or dedifferentiated, which refers to the development of an adjoining high grade nonchondroid neoplasm, usually osteosarcoma or malignant fibrous histiocytoma. It is rare in kids and ought to be differentiated from the chondroblastic number of osteosarcoma. Site: the widespread sites are the pelvis, ribs and proximal ends of femur and humerus. There is proof of cartilaginous matrix mineralization which can be stippled, nodular or conglomerate (popcorn) sometimes displaying rings or arcs. As chondrosarcomas are sluggish growing tumors, reactive changes occur within the normal bone, so that as endosteal resorbtion takes place, periosteal new bone is laid down and bone enlargement happens. Deep endosteal cortical scalloping (greater than two-thirds) is suggestive of chondrosarcoma as opposed to chondroma. Most of the peripheral chondrosarcomas most likely come up from benign osteochondromas. The distinction between energetic osteochondroma and low-grade chondrosarcoma can be extraordinarily difficult. Radiologically, there could also be destruction of part of a well-formed calcified cap or ossified stem of such a structure. Most osteochondromas have cartilage caps less than 5 mm thick and a cap in extra of 20 mm is likely to be malignant. Unfortunately the broad separation between these figures makes this observation of limited worth. Metastases elsewhere, particularly to the skeleton, are rare; similarly regional lymph nodes are also solely rarely concerned. The prognosis is better for peripheral tumors in the limbs than with central tumors. Failure to remove the complete tumor leads to native recurrence and infrequently breakdown of the overlying skin. Clinical image: Pain, swelling and pathological fractures are the widespread presenting options. Site: the tubular bones are extra incessantly involved in younger sufferers, the flat bones in older patients. Almost 50% of these tumors come up within the lower limbs, significantly around the knee. The femur, tibia and humerus account for roughly two thirds of the tumors and the classical location inside these bones are the condyles of the femur and the epicondyles of the humerus. The majority develop primarily in bone and will either be medullary or periosteal in location, whereas a number of come up primarily in delicate tissue and cause secondary bone modifications. Metastases occur to the lungs, central skeleton and viscera in a big share of instances. The zone of transition could differ from slender to diffusely permeative in highly aggressive tumors.
Mamaerie (Papaya). Diltiazem.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96494
First is pyelosinus and pyelovenous backflow and second is enhanced absorption of fluid from the tubules medicine game diltiazem 60 mg buy. There is sufficient proof to present that preglomerular arteriolar resistance develops in acute obstruction treatment kawasaki disease purchase diltiazem 60 mg with mastercard. This resistive index measure by Doppler has been used with variable success to affirm intrarenal vascular resistance in acute obstruction symptoms ibs cheap 180 mg diltiazem free shipping. After a quantity of days of whole ureteric obstruction, less glomerular filtrate is produced so the intrapelvic pressure begins to fall. The indicators indicative of acute obstructive course of are (i) prolonged dense nephrogram, (ii) renal enlargement, (iii) dilatation of the accumulating system, (iv) delayed pyelogram, (v) ureteric dilatation, and (vi) pyelosinus extravasation. Chapter one hundred ten Imaging of Obstructive Uropathy and Diseases of Ureter 1741 If the obstruction is mild, then the nephrogram and calyceal opacification could additionally be regular with minimal dilatation of the ureter. The nephrogram may demonstrate faint radial striations because of distinction within the accumulating ducts and tubules. The opacification of calyces and ureter is delayed and relies upon upon the diploma of obstruction. A fully obstructed kidney that has turn into anuric might not show any opacification of the collecting system; nonetheless as quickly as the opacification of the amassing system begins, additional radiographs are required to demonstrate the location of obstruction. For taking further radiographs, the rule of eight may be helpful to forestall a number of exposures. Unrelieved obstruction with continued extravasation of urine might end result to a retroperitoneal collection referred to as urinoma. Plain film (A) 5 minute movie (B) and 1 hour film (C) exhibits more and more dense left nephrogram. Another downside is its inability to reliably distinguish gentle hydronephrosis from regular or distinguished extrarenal pelvis. The demonstration of ejection of the urine from ureter into urinary bladder excludes total obstruction. Because of technical limitations and inconsistent findings in partial obstruction, evaluation of ureteral jets has limited medical usefulness. Duplex and Color Doppler Sonography Investigations with duplex and colour Doppler ultrasound have yielded advances in three areas: 1. Detecting high grade acute ureteric obstruction through evaluation of ureteral jets. Establishing renal resistive index as an unbiased hemodynamic measure of urinary obstruction. In certain cases normal renal vessels produce separation of the renal sinus echopattern which might mimic gentle pelvicaliectasis. In this case, color Doppler provides a quick and efficient distinction between these two situations. Establishing the etiology of ureteral obstruction when different investigations have failed. Gradual opacification of the medulla follows over minutes to hours, resulting in persistent homogenously dense or diffusely mottled nephrogram. If obstruction is unrelieved, the medullary pyramids may very well turn out to be extra densely opacified then the cortex, creating the reverse corticomedullary nephrogram. In a minority of sufferers, the trigger of obstruction will not be seen as there will not be an intraluminal or periureteral mass. Secondary signs of obstruction embrace stranding of perinephric fat, dilatation of intrarenal amassing system, and unilateral increase in cortical thickness. In obstruction, activity within the parenchyma might rise at a slower fee and persist for a longer time than the nonobstructed kidney. Radionuclide renography nonetheless lacks precise anatomical delineation of obstruction in addition to capability to outline the trigger of obstruction. Its main use is within the differen tiation of a dilated nonobstructed system from a partially obstructed system. If obstructed, no or partial response to the diuretic problem is seen relying on the severity of obstruction. Axial part at the stage of kidneys (A) shows minimal calyceal separation and perinephric stranding on left facet and decrease part at the degree of bladder (B) shows obstructed calculus in lower ureter (arrow) 1744 Section four Genitourinary Imaging that features stones. A grossly hydronephrotic kidney may be seen as a delicate tissue mass within the renal fossa. The ureter turns into dilated proximal to the obstructing lesion, elongated and tortuous, and in excessive instances it might resemble a phase of small intestine. The kidney measurement is small in untreated full obstruction nevertheless lengthy standing partial obstruction can outcome in enlargement of the collecting system and kidney. The nephrographic density could additionally be regular, faint or none depending upon the residual functioning parenchyma. The crescents are skinny, curved collections of contrast denser than the nephrogram, positioned within the medulla. They characterize realigned amassing tubules operating perpendicular to their usual orientation. The opacification of extraordinarily thin parenchyma over the dilated calyceal sac produces a "rim" or shell nephrogram. As distinction medium enters the dilated system, it glides to the dependent portion of calyces. With the patient supine, rounded puddles of contrast appear sixteen Sonography Ultrasound is highly dependable within the detection of chronic ureteral obstruction by demonstrating pyelocaliectasis with reported sensitivities ranging from ninety three to 100 percent. Ultrasound may show falsepositives as the collecting system may appear dilated in sufferers with extrarenal pelvis, vesicoureteric reflux, and protracted change as a outcome of obstruction that has been relieved. Abnormal renal dimensions, various diploma of parenchymal thinning and pyelocaliectasis are seen. Hydronephrosis with parenchymal signs of pyelonephritis, perinephric abscess or thickened renal pelvis can recommend pyonephrosis. To localize the accumulating system earlier than percutaneous nephrostomy or Whitaker take a look at. The corticomedullary distinction normally seen on T1weighted pictures may disappear due to atrophy or destruction of medulla. The dilated pelvicalyceal system is seen as hypointense area on T1 and hyperintense on T2weighted photographs. Obstruction may also be categorized by location as intrarenal, postrenal, supravesical or infravesical. Sonographic steerage facilitates placement of a small caliber needle into the intrarenal amassing system. In the absence of reflux, the obstructive nature of the megaureter should be evaluated by diuretic urogram. Ultrasound usually shows hydronephrosis and dilated renal pelvis with a nondilated ureter. The ureters of a simple ureterocele drain a nonduplex kidney and insert into the bladder at their normal position on the trigone. Ureterocele usually seem on urography and cystography as clean, rounded or ovoid filling defect within the bladder. Circumcaval Ureter Circumcaval ureter results when the supracardinal vein persists and forms the main portion of the inferior vena cava. The typical pattern on urography is a tortuous, dilated proximal right ureter and related hydronephrosis. Primary megaureter could additionally be seen in both kids and adults and usually stays asymptomatic in plenty of cases. Acquired Ureteric Obstruction the causes of acquired ureteric obstruction could be intraluminal or extraluminal. Tissue slough: Necrosed papilla and cholesteaotoma can slough and cause obstruction of ureter with proximal dilatation. Fungus ball: Most fungus balls or mycetomas are attributable to Candida albicans and Aspergillus. Intraluminal Causes Abnormalities might develop inside the ureteral lumen without any attachment to the uroepithelial lining. The widespread causes are calculi, blood clots, tissue slough, fungus ball and international materials. Ureteric Calculus Approximately 90% of urinary stones include calcium (calcium oxalate, magnesium ammo nium phosphate) and 10% are calcium free (uric acid, cystine and xanthine). Oxalate and cystine calculi are radiopaque; nonetheless, pure uric acid calculi are radiolucent on plain radiography.
Areas of intermixed tumor and blood merchandise could show shiny sign depth on T1-weighted photographs treatment in statistics diltiazem 180 mg buy without a prescription. Retrocrural treatment 2nd degree burn discount 180 mg diltiazem otc, paraceliac 897 treatment plant rd 60 mg diltiazem order overnight delivery, gastrohepatic para-aortic, aortocaval, periportal, peripan creatic, exterior and inside iliac groups collectively constitute the retroperitoneal nodes. The retroperitoneal lymph nodes are considered abnormal if their size is greater than 10 mm, besides in the retrocrural house where the higher limit is 6 mm. A variety of retroperitoneal constructions could be confused with enlarged lymph nodes, including unopacified loops of bowel, vascular collaterals, dilated lymphatics and retroperitoneal fibrosis. Benign Lymphadenopathy Benign lymphadenopathy could happen secondary to inflammatory or infectious illness. Enlarged lymph nodes with low density facilities may be seen in pyogenic infections, Whipples illness, lymphomatous or metastatic nodes following radiotherapy and chemotherapy. Enlarged retroperitoneal nodes have also been noticed in 30% of patients with sarcoidosis. Castleman illness is sometimes also related to retroperitoneal lymph node enlargement. This is a progressive disease involving the lung, lymphatic trunks and lymph nodes, typically affecting younger girls of child-bearing age. Sometimes, it could possibly primarily involve retroperitoneum with or without subsequent improvement within the lungs. Lymphomas are homogeneous, with minimal distinction enhancement and relatively low sign depth at T2-weighted images representing densely packed cellular parts. Response to therapy is often indicated by discount within the retroperitoneal lymph node enlargement. In some patients, lymph nodes might turn into hypodense as an acceptable response to therapy with or with out discount in lymph node dimension. Occasionally, there may be post-treatment dystrophic calcification of the lymphomatous masses. It is now thought of the most correct software for the assessment of remedy response and prognosis in sufferers with Hodgkin lymphoma and aggressive non-Hodgkin lymphoma. Metastatic Lymphadenopathy Metastatic lymph nodes show diversified morphological patterns, however the prognosis is usually easy because of the presence of a recognized primary. Neoplasms of the stomach, colon, pancreas, kidney, testis, ovary, uterus, bladder and prostate might all metastasize to retroperitoneal lymph nodes. Calcification in the metastatic nodes recommend mucin producing primary from the ovary or gastrointestinal tract. Lymphatics from the testes drain into ipsilateral lymph nodes, which follow the course of the gonadal veins. Typically, left sided neoplasms unfold to involve lymph nodes in the left renal hilum, as the left gonadal vein drains into the left renal vein. Seminomas could present with cumbersome masses whereas non-seminomatous germ cell tumor usually metastasize to normal sized nodes. Normal lymph nodes lower in sign depth on enhanced T2-weighted and T2-weighted gradient echo pictures, indicating uptake of this contrast agent. These neoplasms are usually derived from mesenchymal cells, neurogenic cells, or embryonic rests and could additionally be benign or malignant. Diagnosis of those tumors is commonly difficult for radiologists and consists of several steps, including determining tumor location (characterizing the retroperitoneal area and figuring out the organ of origin) and recognizing particular features of varied retroperitoneal tumors (evaluating patterns of unfold, tumor components and vascularity). Major vessels and some of their branches are additionally discovered in the retroperitoneal cavity, so that displacement of those vessels could be helpful as well. Before a tumor can be described as primarily retroperitoneal, the possibility that the tumor originates from a retroperitoneal organ must be excluded. This discovering represents mucinous cystadenocarcinoma of the pancreas an organ of origin, the diagnosis of major retroperitoneal tumor turns into probably. Phantom (Invisible) organ sign: When a large mass arises from a small organ, the organ sometimes becomes undetectable. However, falsepositive findings do exist, as in cases of big retroperitoneal sarcomas that involve other small organs such as the adrenal gland. Malignant Neoplasms Malignant tumors of the retroperitoneum are roughly four times extra frequent than benign lesions, in sharp contrast to neoplasms occurring elsewhere within the physique, the place benign lesions predominate. Most main retroperitoneal tumors come up in entrance of the plane of the spine and psoas muscle and regardless of their retroperitoneal location some may project ahead so far as the anterior belly wall. Less generally tumors come up within the paraspinal or posterior pararenal part of the retroperitoneal space. Percutaneous core biopsy is commonly required for the complete histological analysis of these tumors and their distinction from lymphoma. The only constantly effective treatment for primary retroperitoneal sarcomas is operative resection. It is important to determine which organs are definitely or possibly invaded by the tumor for planning appropriate therapy. Primary retroperitoneal sarcomas have a high fee of recurrence after local resection, even when the surgical margins are unfavorable for tumor. Seventy five percent of recurrences sometimes seem within 2 years of preliminary surgical procedure. The best treatment of recurrent retroperitoneal sarcomas is additional surgical resection. Thereafter, all patients should endure annual imaging as a end result of recurrences of low- and high-grade tumors could appear late in some sufferers. The lumen of the duodenum is stretched towards the mass, and the wall of the duodenum seems embedded in the mass at the contact surface (arrow). Histopathology revealed a diagnosis of poorly-differentiated liposarcoma imperceptibly with adjacent normal fat and normally displace rather than invade adjacent organs. These findings embody identification of sentimental tissue septa greater than 2 mm thick inside a fatty retroperitoneal mass, septal irregularity or bulging and obvious enhancement. Any non-fat containing retroperitoneal malignancy could have this appearance Malignant Fibrous Histiocytomas Malignant fibrous histiocytomas are high grade connective tissue tumors. They are multilobulated, infiltrative, unencapsulated however deceptively nicely circumscribed plenty. Although both myxoid stroma and necrosis have related T1 and T2 signal intensity, differentiation could additionally be possible as myxoid stroma shows delayed enhancement in distinction to the nonenhancing necrotic areas. Other Malignancies Fibrosarcomas and neurofibrosarcomas are usually heterogeneous and thus similar in appearance to leiomyosarcomas, some liposarcomas and malignant fibrous histiocytomas. Rhabdomyosarcomas are uncommon, heterogeneous tumors, also seen in pediatric sufferers. Benign Neoplasms Most benign lesions originate from neural tissue or neural crest remnants (neurofibroma, schwannoma, ganglioneuroma, and paraganglioma). Hemangioma, lymphangioma, lipoma, teratoma and desmoid tumors are the other benign tumors encountered in the retroperitoneum. The linear, low sign depth areas, having a somewhat whorled appearance (arrow), correspond to bundles of Schwann cells and collagen fibers throughout the mass Paragangliomas Majority of paragangliomas (extra-adrenal pheochromocytoma) lie in the retroperitoneum, in the quick paraaortic area, from the level of the adrenal glands to the aortic bifurcation. Paragangliomas are homogeneous when small, however turn out to be increasingly heterogeneous as they grow because of central necrosis, hemorrhage and even calcification. Neurogenic Tumors Neurogenic tumors are sometimes located adjacent to the vertebral column or deep to the psoas muscles. At histopathological evaluation, this finding corresponds to bundles of Schwann cells and collagen fibres within the mass. Varying levels of contrast enhancement in neurogenic tumors have been reported, from slight to reasonable to marked with delayed heterogeneous uptake of contrast. These enhancement options are defined by the presence of abundant myxoid materials in these tumors, resulting in delayed progressive accumulation of distinction material within the extracellular space. Retroperitoneal neurofibromas are generally seen in sufferers with neurofibromatosis. Ganglioneuromas come up from sympathetic ganglia and are composed of mature Schwann cells, ganglion cells and nerve fibers. Predominantly children and young adults (60% of cases) are affected and the prognosis is excellent, recurrence being uncommon after surgical resection.
Circumferential mural thickening of the dilated bowel loops with increased attenuation in the mesentery or bowel wall denotes the presence of strangulation medications to treat bipolar 180 mg diltiazem cheap with mastercard. An internal hernia may be identified if a cluster of dilated small bowel loops which seems to be enclosed in a sac is seen in an ectopic location medicine 0027 v buy 180 mg diltiazem amex. A markedly dilated medicine administration purchase 60 mg diltiazem with amex, fluid crammed bowel section with abrupt tapering ends denotes a closed loop obstruction. These present comparatively little dilatation of the proximal bowel and are at larger threat for strangulation. A goal appearance in crosssection with a bowelwithin-bowel look on longitudinal scans suggests a diagnosis of intussusception. Intussusceptions involving the colon which are four cm in size or longer, have proximal dilatation or mural thickening ought to be rigorously evaluated for an underlying neoplasm. Shifting phenomenon is seen on rolling the patient to left lateral place as free air rises to the highest portion of proper hypochondrium. Enhancement of peritoneal stripe refers to increased echogenicity and thickening of the peritoneal stripe as a end result of free intraperitoneal air with associated dirty shadowing. Preoperative localization of the positioning of perforation is beneficial for the surgeon, with the laparoscopic method at present getting used for many surgical procedures as an alternative of open surgery. Other direct signs are the presence of extraluminal air or discontinuity of the bowel wall. Careful analysis of anterior peritoneal surfaces of liver and midabdomen as well as of peritoneal folds must be done, in order not to overlook a small amount of extraluminal air. A large amount of intra peritoneal air often indicates gastroduodenal perforation, apart from bowel perforation brought on by obstruction or an endoscopic procedure. Air within the lesser sac can be seen in posterior perforation of stomach or duodenum, or much less generally, from perforation of transverse colon. Free air confined to the intrahepatic ligamentum teres is usually as a end result of gastroduodenal perforations. Air trapped within the mesenteric folds is found in colon and small bowel perforation, but seldom in gastric perfo ration. Retro peritoneal air is brought on by perforation of extraperitoneal websites of gastrointestinal tract viz. Mesenteric Ischemia Bowel ischemia or infarction is a standard however advanced disorder with a plethora of primary causes and a broad range of clinical and pathological manifestations. Acute mesenteric ischemia is subsequently a diagnostic challenge significantly in view of its excessive mortality price which ranges from 50�90% relying upon the cause and degree of bowel wall injury. A great amount of extraluminal air is seen adjacent to the perforation with extension of inflammation into the proper gluteal region and formation of an abscess. This was a case of carcinoma cecum with perforation 1116 Section three Gastrointestinal and Hepatobiliary Imaging microangiopathies or the antiphospholipid antibody syndrome. Venous occlusions could additionally be caused by infiltrative, neoplastic or inflammatory conditions or hypercoagulable states. The manifestation could range from a selflimiting superficial ischemia involving the watershed zones to a diffuse ischemic harm to the entire bowel-"shock bowel"40. Other causes of bowel ischemia embody neoplasms, bowel obstruction, stomach inflammatory circumstances, trauma, medication, chemotherapy, radiation and corrosive damage. The imaging look in a given case will therefore depend upon the etiology in addition to the diploma of ischemia. Plain films reveal the characteristic thick-walled dilated loops with thumb-printing in only 20�30% of instances. The arterial occlusion/narrowing in addition to the venous occlusion could be readily detected. In addition, involvement of a long segment of bowel or each small and huge bowel with skip segments are options of small vessel illness. The most typical discovering of mesenteric ischemia is bowel wall thickening though this characteristic strongly depends on the diploma of bowel distension. Mural thickening is commoner with ischemic colitis and with veno-occlusive disease but is rare in arterio-occlusive disease where the concerned segment of bowel might show dilated, fluid-filled loops with paper-thin partitions. The bowel wall could present a striated look because of the presence of submucosal edema or hemorrhage. In complete arterial occlusion, there may be absence of the normal enhancement of the bowel wall. Conversely, in nonocclusive ischemia there may be irregular persistent mural enhancement. However, in massive bowel ischemia, pericolonic streakiness could additionally be as a result of superinfection of the ischemic phase. Vascular Causes Vascular conditions that will present as acute abdomen embrace rupture of an aortic aneurysm, spontaneous aortic occlusion, acute hemorrhage and hepatic or splenic vascular occlusion. Aneurysmal dilatation of the stomach aorta is rare before the age of fifty with common age on the time of analysis being 65�70 years. An belly aortic aneurysm is defined as an aortic diameter of three cm or more42 whereas a diameter of 5. Presence of a pulsatile mass and sudden hypotension in the scientific setting of acute ache stomach suggests the prognosis of a ruptured aortic aneurysm. Signs predictive of impending rupture are as follows: zz Draped aorta sign-seen with contained leak. There is associated thrombus as nicely as a peripheral rim of hyperdensity because of the surrounding hematoma therapy. Rare causes of acute stomach embrace hepatic vein thrombosis (acute Budd�Chiari syndrome) and portal vein thrombosis. Absence of flow or move in an abnormal course in all or part of the hepatic veins could also be seen. Visualization of an echogenic adnexal ring separate from the ovary that has prominent peripheral circulate on colour Doppler is extremely suggestive of ectopic gestation. Corpus luteum is a useful guide whereas looking for an ectopic being pregnant and is normally seen within the ipsilateral ovary in 70�85% instances. In adults, a cyst or mass, incessantly a cystic teratoma, is current within the ovary present process torsion. Sonographic findings embrace an enlarged ovary with peripherally distributed follicles, an related cyst or mass, with diminished or absent central venous flow on Doppler. On imaging, hemorrhagic ovarian cysts can mimic a wide range of stable and combined solid-cystic masses. Pregnancy increases the risk for venous thrombosis as a result of stasis, alteration in coagulation elements and by almost tripling the diameter of the ovarian veins. In 90% of cases, the right ovarian vein is concerned as a outcome of dextrotorsion of the uterus. Diverticular disease of the colon affects 65% of the Western inhabitants by the age of sixty five years, and diverticulitis finally develops in up to 25% of people with diverticulosis. Plain radiographs present marked colonic dilatation (>8 cm) significantly of the transverse colon as this is the least dependent part of the large bowel in the supine position. A hypodense space with an air�fluid degree is seen in anterior cortex suggestive of renal abscess. In addition, perinephric assortment with air can be visualized colon full of air, fluid and blood with a distorted or absent haustral sample and irregular, nodular wall. Acute Pyelonephritis Acute pyelonephritis is the bacterial or fungal an infection of the renal parenchyma and collecting system. Emphysematous pyelonephritis normally happens in sufferers with poorly controlled diabetes with the most typical infecting organism being Escherichia coli. It can present details about measurement, localization and chemical composition of the stone. Epiploic appendagitis is due to torsion of an epiploic appendage leading to venous occlusion and ischemia. The condition manifests as acute left decrease quadrant pain, predominantly in males within the 4th�5th decades of life. Acute Urinary Colic Impacted ureteric stone is the commonest reason for acute postrenal obstruction.
The medical signs suggestive of urethral harm in a male patient with pelvic trauma embrace gross hematuria treatment concussion generic diltiazem 180 mg, blood at urethral meatus medicine vials cheap diltiazem 60 mg with mastercard, incapability to void symptoms 2 discount 180 mg diltiazem visa, swelling or hematoma of the perineum or penis and a high using prostate on per rectal examination associated with pelvic fracture. There is a high incidence of related bowel 1768 Section 4 Genitourinary Imaging blood at meatus, hematuria, labial edema, vaginal bleeding or urine leak per rectum. Classification Based on findings of urethrography, the next forms of urethral accidents have been described by Goldman et al. Blunt Urethral Trauma Urethral accidents are categorised anatomically as anterior or posterior urethral accidents. Posterior urethral damage occurs in 4�14% of patients with pelvic fracture and up to 20% of these have associated bladder laceration. However, more generally, anterior urethral accidents could also be iatrogenic because of instrumentation. This is due to disruption of puboprostatic ligaments and hematoma in retropubic and perivesical spaces. Contrast extravasation will be seen adjoining to the posterior urethra and sometimes into the pelvic extraperitoneal house. Anterior Urethral Injury Straddle accidents ensuing from the affected person falling astride a blunt object or direct blow to the perineum might result in anterior, largely bulbous, urethral accidents. More generally, anterior urethral accidents may be iatrogenic because of instrumentation. In partial rupture, extravasation of distinction occurs on urethrogram but continuity of the urethra is preserved. Bladder neck injuries contain inner sphincter and therefore are handled surgically to prevent development of incontinence. Evaluation earlier than Delayed Urethroplasty z Management of Urethral Trauma Type 1 injuries are managed conservatively with placement of a urethral or suprapubic catheter. This enables the surgeon to decide between a transperineal and transpubic method for urethroplasty. Penetrating Injury Penetrating trauma to the urethra could also be secondary to knife or gunshot wounds. Iatrogenic Injury Iatrogenic urethral injury may end result from pelvic surgery, urethral instrumentation or indwelling catheters. Excretory urography or cystourethrography could show extravasation of contrast on the website of rupture. Remarkable progress has since been made in defining the structure and function of the adrenal gland. Adrenal glands are small but their widespread involvement in many disease processes has made cross-sectional imaging modalities essential to detect irregular morphological and useful alterations. Radiology additionally performs a crucial position within the characterization of adrenal mass lesions. Therefore, you will need to first perceive the conventional anatomy and useful traits of the adrenal gland. Zona glomerulosa constitutes 10�15% of the cortex and secretes mineralcorticoids, aldosterone being crucial. Zona fasciculata constitutes 80% of the cortex and secretes glucocorticoids, whereas zona reticularis contributing solely 5�10% of cortex, secretes androgens. Zona glomerulosa is especially concerned in aldosterone biosynthesis whereas fasciculata�reticularis zone is the positioning for cortisol and androgen biosynthesis. The adrenal medulla secretes epinephrine and norepinephrine, which form an integral a half of sympathetic autonomic nervous system and play an important function within the regulation of vital features and lots of metabolic processes. The proper adrenal is pyramidal in form and its relations are liver laterally, upper pole of right kidney inferiorly, proper crus of diaphragm posteromedially and inferior vena cava anteromedially. The left adrenal gland is crescent-shaped and its relations are higher pole of left kidney posterolaterally, left crus of diaphragm posteromedially, anteriorly abdomen in upper two-third and pancreatic physique with splenic vessels in decrease one-third. Each adrenal gland receives its blood supply from three arteries, particularly superior adrenal artery a department of inferior phrenic, middle adrenal artery arising from descending aorta and inferior adrenal artery, a branch of renal artery. There is a single adrenal vein on either side, the proper adrenal vein drains into inferior vena cava and left one into left renal vein. The cortex types virtually 90% of complete adrenal mass; the medulla contributes solely 10%. Adrenal venous sampling may be beneficial in sufferers with aldosteronism, both for distinguishing unilateral from bilateral disease and for localizing unilateral tumor. However, this technique is invasive, techni cally troublesome to carry out and requires lengthy fluoroscopy time with resultant excessive radiation dose and needs hospitalization. Procedural complications include adrenal infarction, adrenal vein thrombosis, adrenal hemorrhage, hypotensive crises and adrenal insufficiency. Therefore, adrenal venous sampling is finest reserved for sufferers with equivocal findings on crosssectional imaging modalities. Integrated information obtained from anatomic and functional imaging is important for characterization of adrenal illness. Major ones requiring therapy occur in 3�5% of the patients and embody hemorrhage and pneumothorax. Therefore, ultrasonography is seldom indicated for adrenal lesion, though large adrenal mass may be detected incidentally during stomach ultrasound examination. Ultrasound is, howe ver, useful in evaluation of suspected adrenal hemorrhage in neonates. It may be used as a screening modality in suspected pheo chromocytoma, as a outcome of the simple availa bility of the examination. Small adrenal lesions may be detected and accurate density measurements of lesions may be accomplished. While evaluating adrenal glands for suspected hyperplasia or adenoma, in a clinical setting of functioning tumors. The finest method is to use 2D or 3D gradientecho sequences, with out fats suppression. Serial post-gadolinium gradient echo may be used for benign vs malignant differentiation. T2-weighted imaging hence is most useful within the seek for pheochromocytomas which have a excessive fluid content. T2-weighted sequences additionally complement benign vs malignant differentiation, though substantial overlap exists. It has demonstrated a high-sensitivity, specificity and general accuracy for detecting adrenal metastases in patients with malignancy. The scientific options depend on the kind of hormone produced and its target organs. It presents an simply recognizable scientific picture of truncal weight problems, moon facies, cutaneous striae, buffalo hump, hypertension, muscles weak spot, fatigability, osteoporosis, profound emotional adjustments and amenorrhea in girls. The adrenal illnesses could also be thought-about under the following three teams: Group I: Adrenal hyperfunctional illnesses. The adrenals show modifications of hyperplasia in the form of smooth thickened limbs or multiple small nodules of various size involving one or each limbs. The presence of necrosis, hemorrhage, and calcification favored a prognosis of carcinoma. It is attributable to adrenal adenoma in about 80% of sufferers while adrenal gland hyperplasia in the remaining. Adrenal carcinoma is extremely uncommon, accounts for less than 1% of patients, as a explanation for aldosteronism. In patients with unilateral adenoma, unilateral adrenalectomy is the therapy of selection. On the opposite hand, circumstances of bilateral adrenal gland hyperplasia are treated medically with pharmacological agents. Bilateral adrenal visualization earlier than fifth day suggests adrenal gland hyperplasia while unilateral adrenal visualization before fifth day signifies an adenoma. Androgen producing tumors are uncommon and embrace adenoma or carcinoma, and happen in both males and females at a later age. In basic, in adults a better proportion of malignant tumors lead to adrenogenital syndrome than benign lesions. Occasionally adrenal and gonadal venous sampling could additionally be essential to locate the supply of extreme androgens. Pheochromocytoma or precocious puberty relying upon the age and sex of the patient. The adrenal causes of androgen excess embrace congenital adrenal hyperplasia in kids and virilizing tumors (adenoma or carcinoma) in adults. Each different enzyme deficiency leads to a unique form of congenital adrenal hyperplasia.
Sometimes tears might not present T2 hyperintensity due to medications migraine headaches diltiazem 180 mg discount fast delivery granulation or fibrosis and appear to be regular symptoms zinc deficiency husky diltiazem 180 mg buy without prescription. Although less particular treatment for depression diltiazem 180 mg cheap mastercard, data of secondary signs of rotator cuff tear is beneficial in such difficult instances. Tendons may be fully nonvisualized because of musculotendinous retraction in full tears. But this mobility comes on the expense of stability because the joint architecture which permits most mobility additionally predisposes it to dislocation. Glenohumeral joint is relatively shallow with a large humeral head compared to glenoid fossa. Anterior instability is commonly related to anteroinferior labral tear with or without glenoid rim fracture (Bankart lesion). Multidirectional nontraumatic instability is seen in younger without history of trauma. It is also useful for diagnosing associated instability and capsulolabral disorders. Imaging Techniques for Labral Tears the shape of labrum varies from particular person to particular person (triangular, rounded, blunted, crescent shaped, etc). Few horizontal notches and vertical clefts alongside anterior facet of labrum are thought of regular. However, one 3246 Section 7 Musculoskeletal and Breast Imaging study by Chandnani et al. Identification of those lesions is necessary as they predispose to recurrent dislocation with minimal trauma and may have an result on surgical planning. Loose our bodies can happen in joint from detached avulsed articular cartilage fragment. However, a big capacious anterior pouch/subscapularis bursa is a frequent secondary finding in sufferers with recurrent anterior subluxation. A close scrutiny of rotator cuff interval should also be accomplished in all sufferers of medical instability with rotator cuff tear as capsule is weak on this area. The retracted tendon fibers (black arrow) and marrow edema at the lesser tuberosity (arrowhead) could be seen. A redundant posterior capsule indicates shoulder instability (long arrow) sometimes seen in younger individuals concerned in sports exercise requiring overhead movement of humeral head like bowlers. They are believed to be attributable to repetitive contact of humeral head with posterosuperior labrum. This unique classification was later expanded on foundation of arthroscopic findings; however, their clinical implication is questionable. They are troublesome to diagnose however necessary to establish as they respond properly to arthroscopic restore. Labral tears may be related to labral cysts or ganglia which can cause compression neuropathy. These kind due to a technique valve mechanism resulting in accumulation of joint fluid within them. Subscapularis tears are seen after anterior dislocation over 40 years of age and after posterior dislocation at any age. The most important regular variation is a deficient attachment of labrum in the anterosuperior quadrant of glenoid (sublabral foramen or recess). Contrast in sublabral recess is seen as a skinny line with easy margins that runs along the glenoid. Contrast in a tear has irregular margins, globular shape and is seen to enter into labral substance. Bicipital tendinopathy may happen in sufferers with glenohumeral instability and attrition on the groove. Morphologic abnormalities similar to fraying, flattening and absence of tendon could someday be identified. Disproportionate quantity of fluid in bicipital tendon sheath as in comparison with the joint fluid may recommend bicipital abnormality, i. Bicipital Tendon Dislocations Bicipital tendon dislocation usually occurs with the persistent rotator cuff tears that have prolonged to involve the subscapularis tendons. When all of the three structures are disrupted, tendons of long head of biceps dislocates medially posterior to subscapularis tendon into the joint, where it could be mistaken for a indifferent anterior labrum. Rarely when subscapularis tendon stays intact, with the disruption of different two ligaments, biceps tendon displaces extra-articularly, anterior to subscapularis muscle. Suprascapular Nerve Entrapment Suprascapular nerve passes via supraspinatus notch to enter supraspinatus fossa beneath supraspinatus muscle tissue. Further posteriorly it passes by way of spinoglenoid notch to enter into the intraspinatus fossa. Compression of nerve on the stage of suprascapular notch leads to atrophy of each muscle tissue and compression on the level of spinoglenoid notch ends in atrophy of infraspinatus muscle only. Patients present with ache and paresthesia in axillary nerve distribution and muscle atrophy of teres minor and main muscular tissues. Calcification of rotator cuff most commonly happens in supraspinatous tendon however can occur in different tendons. Loose bodies happen in glenohumeral joint and subacromial bursa which appear isointense to bone or hypointense on T2W photographs. Immunocompromised standing and pre-existing degenerative joint illness will increase danger of septic arthritis. However, typical systemic and native signs could also be absent in indolent infections like tuberculosis. T1W coronal part (B) exhibits globular area of hypointense signal (arrow) within the supraspinatus tendon suggestive of calcific tendinitis Chapter 196 Magnetic Resonance Imaging of Shoulder and Temporomandibular Joints 3251 decide up early marrow or delicate tissue modifications. Further progression of disease leads to cartilage destruction manifesting as joint area narrowing and marginal erosion of naked space. Subchondral bone changes in type of edema, subchondral cyst formation and bone destruction observe when illness turns into subacute. Osteomyelitis, bone destruction and joint ankylosis are options of chronic septic arthritis. Tuberculosis of shoulder joint is rare and has indolent clinical presentation. Patients often presents with pain and restriction of movement for lengthy period. Frequent benign lesions comprise osteochondroma, chondroma, chondroblastoma and giant cell tumor. It can be differentiated from osteoarthritis by sign abnormality confined to the humeral head and sparing of glenoid. Metadiaphyseal lesions could show classical serpiginous low intensity line surrounding excessive depth center (in chronic infarcts) and high-intensity rim in more acute infarcts. Axial aircraft is used for localization of condyle and planning of sagittal and coronal pictures. Coronal pictures are acquired alongside the horizontal long axes of condyles in closed mouth position. The inversion restoration image reveals darkish signal because of fat saturation (B) aircraft of imaging. The most well-liked sequences are T1 spin echo (shows fat as bright), T2 turbo spin echo (fluid sensitive) and proton density photographs. Functional joint dynamics at incremental mouth opening may be shown with small flip angle gradient echo imaging. The disk is composed of avascular fibrous connective tissue which merges with peripheral capsule. The head opposed to articular eminence with thin zone of disk interposed between the 2 (last frame upper row). Note growth of the posterior delicate tissues as mouth opens roughly 18 mm in anteroposterior dimension and 20 mm in mediolateral extension. Two localized thickenings are current in the disk, referred to as anterior and posterior bands. Consequently the disk is 2 mm thick in its anterior part, 1 mm centrally and three mm in its posterior half.






