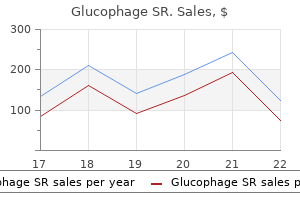
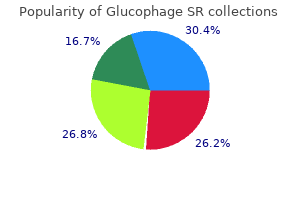
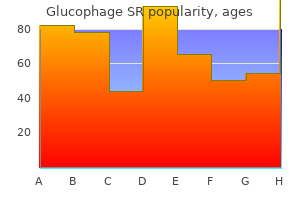
Glucophage SR
Glucophage SR
Glucophage SR dosages: 500 mg
Glucophage SR packs: 90 pills, 120 pills, 180 pills, 240 pills, 360 pills

Chloroprocaine Agents Used Primarily to Anesthetize Mucous Membranes and Skin Some brokers are useful as topical anesthetic brokers on the pores and skin or mucous membranes symptoms after hysterectomy 500 mg glucophage sr generic visa, though too irritating or too ineffective to be utilized to the eye symptoms acid reflux cheap glucophage sr 500mg without prescription. Dyclonine Mepivacaine Dyclonine hydrochloride is quickly absorbed via the skin and mucous membranes medicine zolpidem glucophage sr 500mg purchase with visa. The increased toxicity of mepivacaine within the neonate is said to ion trapping of this agent because of the decrease pH of neonatal blood and the pKa of mepivacaine, somewhat than to its slower metabolism in the neonate. Its onset of motion is similar to, and its period barely longer (~20%) than, that of lidocaine in the absence of a coadministered vasoconstrictor. It is simply too irritating to be used on the eye or in the nose, however an otic answer containing chloroxylenol is marketed. Anesthetics With Low Aqueous Solubility Some local anesthetics have low aqueous solubility and consequently are absorbed too slowly to trigger classical local anesthetic toxicity. Agents for Ophthalmic Use Anesthesia of the cornea and conjunctiva may be obtained readily by topical application of native anesthetics. However, a lot of the native anesthetics which have been described are too irritating for ophthalmological use. For use in ophthalmology, these native anesthetics are instilled a single drop at a time. Long-term administration of topical anesthesia to the attention has been associated with retarded therapeutic, pitting, and sloughing of the corneal epithelium and predisposition of the eye to inadvertent harm. For problems with drug supply, pharmacokinetics, and toxicity unique to drugs for ophthalmic use, see Chapter sixty nine. Second, neurophysiological responses to ache and stress may be modified beneficially. However, local anesthetics have the potential to produce deleterious side effects. Proper selection of a neighborhood anesthetic and care in its use are the first determinants in avoiding these issues. There is a poor relationship between the quantity of local anesthetic injected and peak plasma levels in adults. This dialogue summarizes the pharmacological and physiological consequences of the use of native anesthetics categorized by method of administration. A more comprehensive dialogue of their use and administration is presented in textbooks on regional anesthesia (Cousins et al. The shrinking of mucous membranes decreases operative bleeding whereas improving surgical visualization. Maximal safe complete dosages for topical anesthesia in a wholesome 70-kg adult are 300 mg for lidocaine, one hundred fifty mg for cocaine, and 50 mg for tetracaine. Peak anesthetic impact following topical application of cocaine or lidocaine occurs inside 2�5 min (3�8 min with tetracaine), and anesthesia lasts for 30�45 min (30�60 min with tetracaine). Local anesthetics are absorbed rapidly into the circulation following topical utility to mucous membranes or denuded skin. Concentrations in blood after instillation of native anesthetics into the airway are nearly the same as those following intravenous injection. Surface anesthetics for the skin and cornea have been described earlier within the chapter. The efficacy of every of these combinations lies in the fact that the combination has a melting point lower than that of either compound alone, current at room temperature as an oil that may penetrate intact skin. These mixtures are effective for procedures involving skin and superficial subcutaneous buildings. These mixtures should not be used on mucous membranes or abraded skin, as rapid absorption across these surfaces could end in systemic toxicity. Tetrodotoxin is found in the gonads and other visceral tissues of some fish of the order Tetraodontiformes (to which the Japanese fugu, or puffer fish, belongs); it also happens within the pores and skin of some newts of the family Salamandridae and of the Costa Rican frog Atelopus. Given the right circumstances of temperature and lightweight, the Gonyaulax might multiply so rapidly as to discolor the ocean, causing the condition often identified as pink tide. Shellfish feeding on Gonyaulax right now turn out to be extraordinarily toxic to people and are liable for periodic outbreaks of paralytic shellfish poisoning (Sakai and Swanson, 2014; Stommel and Watters, 2004). Both toxins, in nanomolar concentrations, particularly block the outer mouth of the pore of Na+ channels within the membranes of excitable cells. Not all Na+ channels are equally delicate to tetrodotoxin; some Na+ channels in cardiac myocytes and dorsal root ganglion neurons are resistant, and a tetrodotoxin-resistant Na+ channel is expressed when skeletal muscle is denervated. Both toxins have brought on deadly poisoning in people due to paralysis of the respiratory muscles; therefore, the therapy of severe cases of poisoning requires help of respiration. If the affected person survives paralytic shellfish poisoning for 24 h, the prognosis is nice. The period of infiltration anesthesia may be approximately doubled by the addition of epinephrine (5 g/mL) to the injection solution; epinephrine also decreases peak concentrations of native anesthetics in blood. Epinephrine-containing options are generally not injected into tissues supplied by end arteries-for instance, fingers and toes, ears, the nostril, and the penis-because of a concern that the ensuing vasoconstriction could trigger gangrene. Tumescent anesthesia is a special case of infiltration anesthesia for which giant doses and volumes of lidocaine and epinephrine are administered (Lozinski and Huq, 2013). This may be done at certainly one of a number of levels: subcutaneously, at main nerves, or at the stage of the spinal roots. The utility of higher concentrations, nevertheless, is proscribed by systemic toxicity and by direct neural toxicity of concentrated local anesthetic options. For a given focus, native anesthetics with lower pKa values tend to have a more rapid onset of action as a outcome of extra drug is uncharged at neutral pH. In distinction, the onset of action of bupivacaine requires about 15 min; solely 5%�10% of bupivacaine is uncharged at this pH. Increased hydrophobicity might be expected to velocity onset by increased penetration into nerve tissue. Local anesthetics may be broadly divided into three classes: � these with a short (20- to 45-min) period of action in combined peripheral nerves, corresponding to procaine; � those with an intermediate (60- to 120-min) period of motion, such as lidocaine and mepivacaine; and � these with an extended (400- to 450-min) period of motion, similar to bupivacaine, ropivacaine, and tetracaine. Block length of the intermediate-acting native anesthetics corresponding to lidocaine could be extended by the addition of epinephrine (5 g/mL). The diploma of block prolongation in peripheral nerves following the addition of epinephrine appears to be related to the intrinsic vasodilating properties of the native anesthetic and thus is most pronounced with lidocaine. A mixed peripheral nerve or nerve trunk consists of individual nerves surrounded by an investing epineurium. When a neighborhood anesthetic is deposited about a peripheral nerve, it diffuses from the outer surface towards the core along a focus gradient. If the volume and focus of native anesthetic solution deposited about the nerve are enough, the native anesthetic eventually will diffuse inward in quantities enough to block even the most centrally situated fibers. The alternative of native anesthetic and the amount and concentration administered are determined by the nerves and the kinds of fibers to be blocked, the required duration of anesthesia, and the scale and well being of the affected person. The medication, concentrations, and doses beneficial are the identical as for infiltration anesthesia. The benefit of subject block anesthesia is that less drug can be used to provide a larger area of anesthesia than when infiltration anesthesia is used. Knowledge of the relevant neuroanatomy obviously is essential for successful area block anesthesia. The areas of sensory and motor block usually begin a number of centimeters distal to the site of injection. Other useful nerve blocks prior to surgical procedures embrace blocks of particular person nerves on the wrist and at the ankle, blocks of individual nerves such because the median or ulnar on the elbow, and blocks of sensory cranial nerves. There are 4 major determinants of the onset of sensory anesthesia following injection close to a nerve: (1) proximity of the injection to the nerve; (2) concentration and volume of drug; (3) degree of ionization of the drug; and (4) time. Addition of 5 g/mL epinephrine slows systemic absorption and therefore prolongs length and lowers the plasma concentration of the intermediate-acting local anesthetics. In this technique, an extremity is exsanguinated with an Esmarch (elastic) bandage, and a proximally positioned tourniquet is inflated to 100�150 mm Hg above the systolic blood stress. The Esmarch bandage is eliminated, and the local anesthetic is injected right into a previously cannulated vein. Pain from the tourniquet and the potential for ischemic nerve injury limit tourniquet inflation to 2 h or much less. However, the tourniquet should remain inflated for at least 15�30 min to forestall poisonous amounts of native anesthetic from entering the circulation following deflation. The following is a quick discussion of the physiological effects of spinal anesthesia relating to the pharmacology of the local anesthetics. Most of the physiological side effects of spinal anesthesia are a consequence of the sympathetic blockade produced by local anesthetic block of the sympathetic fibers in the spinal nerve roots. Although local anesthetic is injected below these levels within the lumbar portion of the dural sac, cephalad spread of the native anesthetic happens with all however the smallest volumes injected.
Diseases
A: Bone marrow aspirate demonstrating elevated iron staining present in a patient with anemia of continual illness symptoms you may be pregnant glucophage sr 500mg safe. This blood smear can be seen in the anemia of continual disease however normally that kind of anemia is normocytic and normochromic medications via g-tube order glucophage sr 500 mg visa. Mild microcytosis and hypochromia can develop as the severity of the underlying situation causing the anemia of persistent illness worsens and iron availability markedly declines medicine vial caps 500mg glucophage sr purchase amex. Bone marrow biopsy from a affected person with pure red cell aplasia before and after remedy with immunosuppressive agents. A: Bone marrow aspirate smear reveals a large erythroblast with intranuclear viral inclusion. This inclusion can resemble a large nucleolus, and the erythroblast cytoplasm could seem darkish blue and contain vacuoles. B: Bone marrow biopsy with early erythroid precursors exhibiting "glassy" intranuclear inclusions (so-called lantern cells; arrows). Other congenital anomalies could happen: skin pigmentation modifications, brief stature, higher limb abnormalities, renal malformations, ophthalmologic problems, hypogonadism, and cardiac malformations. Chromosomal karyotyping of peripheral blood lymphocytes in a affected person with Fanconi anemia. Increased spontaneous chromosomal breakage could also be seen, however on exposure to mitomycin C or diepoxybutane (right side), increased chromosomal breaks and radial chromosomal fusions occur. A: Normoblastic erythroid hyperplasia is current with a predominance of erythroid precursors. Bartonellosis hemolysis can also be related to inclusions of the bacilli within the purple cells. Peripheral blood smear of spherocytic hemolysis due to an inherited membrane abnormality. Increased fragility is indicated by a shift of the curve to the left, and is seen in situations associated with spherocytosis. B: Incubation of the pattern for 24 hours prior accentuates the osmotic fragility of spherocytes, whereas normal cells solely turn into more barely fragile. Peripheral blood smear demonstrating spiculated spheroid cells in a affected person with pyruvate kinase deficiency hemolytic anemia. Elliptocytes and ovalocytes are present on this relatively frequent hereditary common membrane defect. Elliptocytes are elongated with rounded edges (as opposed to sharp edges in sickle cells). A gentle hemolytic anemia is the one medical manifestation, although uncommon patients could have extra severe hemolysis. Hereditary stomatocytosis disorders are because of membrane defects related to altered sodium permeability and may show 10% to 50% stomatocytes on the peripheral blood movie. Peripheral blood smear from a affected person with hereditary pyropoikilocytosis, which is a variant of hereditary elliptocytosis. These morphologic adjustments occur at a lower temperature than with samples from individuals without this disorder. The increased density of the irregularly contracted cells might give the hemoglobin a dark copper colour. The erythrocyte might retain or lose central pallor, depending on the scale and numbers of bites. In some instances, the bite cell may be mistaken for helmet cells, a sort of fragmented erythrocyte. Besides components that produce oxidative hemolysis, bite cells also occur in inherited unstable hemoglobins due to the formation of denatured hemoglobin (Heinz bodies), which are phagocytized in the spleen. Excessive 204 quantities of acidic proteins (often immunoglobulins produced by myeloma cells) trigger a rise in background bluish staining in blood smears. A: the hand on the proper in this image is warmed in a patient with continual chilly agglutinin disease. In the method of purple cell fragmentation, an occasional irregularly contracted erythrocyte, chunk cells, or spherocytes could be seen, however the diagnosis of microangiopathic hemolytic anemia should be made by the morphology of a lot of the cells, which on this case are fragments. Note the severe thrombocytopenia related to peripheral destruction of platelets in microthrombi indicating that the prognosis for this affected person is thrombotic thrombocytopenic purpura or disseminated intravascular coagulation. A: Coronal section through the mind at post-mortem exhibiting a quantity of small hemorrhages (arrows). B: Histologic part from the identical affected person exhibits diffuse microvascular occlusion of arterioles and capillaries. A: Peripheral blood movie demonstrating acanthocytes, alternatively known as spur cells. B: this peripheral blood film demonstrates many acanthocytes in a patient with extreme liver disease and hemolysis. The green cells are granulocytes, the blue cells monocytes, and the pink cells lymphocytes (A). B: the clear sample on the left is normal, and the pattern on the right is from a affected person with hemolysis. The pattern to the right demonstrates the red look of urine as a end result of hemoglobinuria throughout acute hemolysis. This check may be useful in detecting a recent episode of hemolysis that has resolved. First morning urines tend to be darker, in addition to urines taken during intercurrent diseases, due to elevated intravascular hemolysis. Leukoerythroblastic anemia, associated with metastasis to the bone marrow or other myelophthisic illness, corresponding to tuberculosis of marrow. The numerous curved, elongated erythrocytes with sharp factors are classic sickle cells. A composite figure taken from different sickle cell anemia cases showing varied shapes of sickle cells. In this test, entire blood is added to a excessive phosphate buffer with saponin and sodium dithionite, which causes the hemoglobin to turn out to be deoxyhemoglobin. Gallstones extracted from a affected person with continual hemolysis from sickle cell disease. Cholelithiasis also can happen in sufferers with other hereditary hemolytic problems, corresponding to hereditary spherocytosis. A: "Comma" vascular signal: superficial conjunctival vessel that incorporates densely packed sickle cells (arrow). Chest radiographs of the spine reveal central endplate melancholy with sparing of the anterior and posterior margins of the endplate (arrow). Although not pathognomonic, these radiologic findings are seen most frequently in sickle cell disease. In addition, the gastric air bubble occupies most of the region underneath the left hemidiaphragm extending to the left lateral thoracic cage, suggesting the absence of a 222 spleen. The commonest site of skin ulcers in sickle cell anemia is the lower limb, often over bony prominences such because the ankles. They usually characterize vascular occlusion and necrosis of small skin vessels because the initiating occasion, then fail to heal. Few sickle cells are current, and they are inclined to be quick, stubby, and rhomboid-shaped (oat or boat cells). The condensation of Hb crystals in this blood movie produces darkish, blunt protuberances and other distortions. Target cells, irregularly contracted cells, and hemoglobin C crystals are present with microcytosis on this blood smear. Hemoglobin C crystals (arrows) are seen in cells which are in any other case empty of hemoglobin. More frequent are goal cells, irregularly contracted erythrocytes, and microcytosis. Peripheral blood smear in -thalassemia trait could show microcytosis and hypochromia. Multiple morphologic changes including target cells, teardrop cells, and rare fragments may occur. These features can seem equivalent to the morphologic image of iron deficiency. Basophilic stippling can occur in Mediterranean populations with -thalassemia trait and is much less widespread in different populations with this dysfunction.
Although the hemodynamic profile of etomidate may be advantageous treatment room discount 500 mg glucophage sr visa, potential adverse results on steroid synthesis elevate concerns about its use in trauma and critically sick patients (van den Heuvel et al medicine etodolac glucophage sr 500 mg buy otc. Note that the half-times of some drugs similar to etomidate symptoms 5 days before missed period buy generic glucophage sr 500mg online, propofol, and ketamine increase only modestly with extended infusions; others. Ketamine rapidly produces a hypnotic state quite distinct from that of other anesthetics. The administration of ketamine has been proven to reduce the event of tolerance to long-term opioid use. Ketamine sometimes is administered intravenously but in addition is effective by intramuscular, oral, and rectal routes. The onset and length of an induction dose of ketamine are determined by the same distribution/redistribution mechanisms operant for all the other parenteral anesthetics. Norketamine, with ~20% of the activity of ketamine, is hydroxylated and excreted in urine and bile. Ketamine has indirect sympathomimetic activity and produces distinct behavioral results. Ketamine produces profound analgesia, a definite advantage over different parenteral anesthetics. Emergence delirium, characterized by hallucinations, vivid goals, and delusions, is a frequent complication of ketamine that can lead to serious affected person dissatisfaction and can complicate postoperative management. Unlike different anesthetics, induction doses of ketamine typically improve blood strain, coronary heart price, and cardiac output. The cardiovascular results are indirect and are most probably mediated by inhibition of each central and peripheral catecholamine reuptake. Thus, ketamine is a useful drug, along with etomidate, for patients in danger for hypotension during anesthesia. The three barbiturates most commonly used in medical anesthesia are sodium thiopental (not currently marketed within the U. Barbiturates are formulated as the sodium salts with 6% sodium carbonate and reconstituted in water or isotonic saline to alkaline solutions, 10 < pH <11. Table 19�3 lists the frequent barbiturates with their scientific pharmacological properties. All three barbiturates are primarily eliminated by hepatic metabolism and subsequent renal excretion of inactive metabolites; a small fraction of thiopental undergoes desulfuration to the longer-acting hypnotic pentobarbital. Typically, coronary heart rate increases as a compensatory response to a lower blood stress, although barbiturates additionally blunt the baroreceptor reflex. Hypotension may be severe in patients with an impaired capability to compensate for venodilation, similar to those with hypovolemia, cardiomyopathy, valvular coronary heart illness, coronary artery illness, cardiac tamponade, or adrenergic blockade. Induction doses of thiopental lower minute air flow and tidal quantity, with a smaller and inconsistent lower in respiratory fee. Compared to propofol, barbiturates produce a higher incidence of wheezing in asthmatics, attributed to histamine launch from mast cells throughout induction of anesthesia. Short-term administration of barbiturates has no clinically vital effect on the hepatic, renal, or endocrine methods. True allergies to barbiturates are uncommon; however, direct drug-induced histamine launch is often seen. Inadvertent intra-arterial injection of thiobarbiturates can induce a extreme inflammatory and doubtlessly necrotic response that may threaten limb survival. The toxicity of those medication is basically a function of their unwanted effects, and every of the inhalational anesthetics has a singular side-effect profile. Table 21�3 lists the broadly various bodily properties of the inhalational brokers in medical use. Ideally, an inhalational agent would produce speedy induction of anesthesia and rapid restoration following discontinuation. Recommended intravenous dosing for parent- Pharmacokinetic Principles Inhalational brokers behave as gases rather than as liquids and thus require totally different pharmacokinetic constructs to be utilized in analyzing their uptake and distribution. Note that all inhalational common anesthetic brokers besides nitrous oxide and halothane are ethers, and that fluorine replaces chlorine in the growth of the halogenated agents. Blood:gasoline, mind:blood, and fat:blood partition coefficients for the varied inhalational agents are listed in Table 21�3. If an agent is extra soluble in a tissue such as fats, equilibrium might take many hours to reach. This happens as a end result of fats represents a huge anesthetic reservoir that might be crammed slowly because of the modest blood move to fat. Because the brain is well perfused, anesthetic partial strain in brain turns into equal to the partial strain in alveolar gas (and in blood) over the course of a number of minutes. This happens as a end result of the amassed quantities of anesthetic in the fat reservoir will forestall blood (and due to this fact alveolar) partial pressures from falling quickly. Induction of anesthesia may be achieved in less than 10 min with an inhaled focus of 1. Isoflurane has a blood:gasoline partition coefficient considerably lower than that of enflurane. Isoflurane produces a concentration-dependent lower in arterial blood pressure; cardiac output is well maintained; hypotension is the outcomes of decreased systemic vascular resistance. Isoflurane produces vasodilation in most vascular beds, with pronounced results in skin and muscle, and is a potent coronary vasodilator, simultaneously producing increased coronary blood move and decreased myocardial O2 consumption. This drug is particularly effective at depressing the ventilatory response to hypercapnia and hypoxia. Although isoflurane is a bronchodilator, it is also an airway irritant and may stimulate airway reflexes throughout induction of anesthesia, producing coughing and laryngospasm. Sevoflurane produces a concentration-dependent reduction in tidal quantity and increase in respiratory fee in spontaneously breathing sufferers. Biochemical evidence of transient renal damage has been reported in human volunteers (Eger et al. Large medical studies have proven no proof of elevated serum creatinine, blood urea nitrogen, or any other evidence of renal impairment following sevoflurane administration. Desflurane Sevoflurane Desflurane is a extremely volatile liquid at room temperature (vapor stress = 669 mm Hg) and must be stored in tightly sealed bottles. Delivery of a exact concentration of desflurane requires the usage of a specially heated vaporizer that delivers pure vapor that then is diluted appropriately with different gases (O2, air, or N2O). Induction of anesthesia is rapidly achieved utilizing inhaled concentrations of 2%�4% sevoflurane. Desflurane is minimally metabolized; greater than 99% of absorbed desflurane is eliminated unchanged through the lungs. Desflurane produces hypotension primarily by decreasing systemic vascular resistance. Cardiac output is nicely preserved, as is blood move to the main organ beds (splanchnic, renal, cerebral, and coronary) (Eger, 1994). Desflurane causes a concentration-dependent enhance in respiratory price and a lower in tidal volume. However, it also is a powerful airway irritant and may cause coughing, breath-holding, laryngospasm, and extreme respiratory secretions. Because of its comparatively high blood:gasoline partition coefficient, induction of anesthesia and restoration from enflurane are comparatively slow. Fluoride ions are a by-product of enflurane metabolism, however plasma fluoride levels are low and unhazardous. Patients taking isoniazid exhibit enhanced metabolism of enflurane with consequent elevation of serum fluoride. Enflurane causes a lower in arterial blood pressure, the results of vasodilation and despair of myocardial contractility, with minimal results on coronary heart price. Halothane hepatitis may be the result of an immune response to hepatic proteins that turn into trifluoroacetylated as a consequence of halothane metabolism. Those excited about additional data on halothane should seek the guidance of earlier current editions of this e-book. The analgesic property of N2O is a perform of the activation of opioidergic neurons within the periaqueductal grey matter and the adrenergic neurons within the locus ceruleus.
Local anesthetics can bind to other membrane proteins (Butterworth and Strichartz symptoms 14 days after iui 500 mg glucophage sr with amex, 1990) medicine show discount glucophage sr 500 mg online. Procaine is a prototypic ester-type local anesthetic; esters usually are rapidly hydrolyzed by plasma esterases treatment 9mm kidney stones discount glucophage sr 500 mg, contributing to the relatively brief length of action of medicine in this group. There are exceptions, together with benzocaine (poorly water soluble; used solely topically) and the structures with a ketone, an amidine, and an ether linkage. Electrical area (negative inside) exerts a force on these charged amino acid residues, pulling them towards the intracellular aspect of the membrane; depolarization permits them to move outward and provoke a conformational change that opens the pore. On depolarization, each of the four homologous domains sequentially undergoes a conformational change to an activated state. This loop folds over the intracellular mouth of the transmembrane pore in the course of the strategy of inactivation and binds to an inactivation gate "receptor" formed by the intracellular mouth of the pore. A voltage-gated Na+ channel may be considered an antechamber (extracellular funnel) that feeds right into a constricted area (selectivity filter), which opens onto a bigger quantity (central cavity) that has an exit door (gate). The effect of an action potential is to provoke a conformational change within the selectivity funnel area of the channel, moving the constructive costs outward and away from the pore interior. These frequency- and voltage-dependent results of local anesthetics happen as a result of the charged form of the native anesthetic molecule positive aspects access to its binding site within the pore primarily when the Na+ channel is open and because the local anesthetic binds more tightly to and stabilizes the inactivated state of the Na+ channel (Butterworth and Strichartz, 1990; Courtney and Strichartz, 1987; Hille, 1977). Local anesthetics exhibit frequency and voltage dependence to totally different extents depending on their pKa, lipid solubility, molecular measurement, and binding to completely different channel states. Dissociation of smaller and more hydrophobic medication is more rapid, so a higher frequency of stimulation is required to yield frequency-dependent block. Because local anesthetics are weak bases (typical pKa values range from eight to 9), their hydrochloride salts are mildly acidic. This property increases the stability of the native anesthetic esters and the catecholamines added as vasoconstrictors. The major position of the cationic type also was demonstrated by Narahashi and Frazier, who perfused the extracellular and axoplasmic surface of the enormous squid axon with tertiary and quaternary amine native anesthetics and located that the quaternary amines had been active only when perfused intracellularly (Narahashi and Frazier, 1971). Differential Sensitivity of Nerve Fibers For most sufferers, treatment with local anesthetics causes the feeling of ache to disappear first, adopted by lack of the sensations of temperature, contact, deep stress, and eventually motor perform (Table 22�1). Classical experiments with intact nerves showed that the wave within the compound action potential, which represents slowly conducting, small-diameter myelinated fibers, was lowered more rapidly and at decrease concentrations of cocaine than was the wave, which represents rapidly conducting, large-diameter fibers (Gasser and Erlanger, 1929). In general, autonomic fibers, small unmyelinated C fibers (mediating ache sensations), and small myelinated A fibers (mediating pain and temperature sensations) are blocked earlier than the bigger myelinated A, A, and A fibers (mediating postural, contact, strain, and motor information) (Raymond and Gissen, 1987). The preliminary hypothesis was that sensitivity to local anesthetic block will increase with lowering fiber size, according to high sensitivity for pain sensation mediated by small fibers and low sensitivity for motor operate mediated by large fibers (Gasser and Erlanger, 1929). Because a set variety of nodes have to be blocked to forestall conduction, small fibers with intently spaced nodes of Ranvier may be blocked more rapidly during remedy of intact nerves because the native anesthetic reaches a crucial size of nerve more rapidly. Differences in tissue limitations and site of smaller C fibers and A fibers in nerves additionally may affect the rate of local anesthetic action. Consequently, maneuvers that maintain the drug on the nerve prolong the period of anesthesia. Note, however, that epinephrine dilates skeletal muscle vascular beds through actions at 2 adrenergic receptors and due to this fact has the potential to increase systemic toxicity of anesthetic deposited in muscle tissue. There also could additionally be delayed wound healing, tissue edema, or necrosis after local anesthesia. Thus, the usage of vasoconstrictors in native anesthetic preparations for anatomical areas with restricted collateral circulation is averted. Local anesthetics might increase the resting tone and reduce the contractions of isolated human uterine muscle; nonetheless, uterine contractions are seldom depressed instantly during intrapartum regional anesthesia. The hazard of such antagonistic reactions is proportional to the focus of native anesthetic achieved in the circulation. Neuromuscular Junction and Ganglia Local anesthetics also affect transmission at the neuromuscular junction. Central stimulation is followed by despair; death normally is caused by respiratory failure. Under these situations, the focus of the drug in all probability rises so rapidly that every one neurons are depressed simultaneously. Neither propofol nor a quickly performing barbiturate is most popular; each usually have a tendency to produce cardiovascular depression than a benzodiazepine (Chapter 19). For instance, individuals delicate to procaine additionally might react to structurally comparable compounds. Although allergic responses to agents of the amide kind are uncommon, options of such brokers might contain preservatives corresponding to methylparaben that will provoke an allergic reaction (Covino, 1987). Because spinal fluid contains little or no esterase, anesthesia produced by the intrathecal injection of an anesthetic agent will persist until the native anesthetic agent has been absorbed into the circulation. The primary site of motion is the myocardium, the place decreases in electrical excitability, conduction rate, and pressure of contraction occur. However, on uncommon occasions, decrease doses of some native anesthetics will trigger cardiovascular collapse Toxicity the metabolic fate of native anesthetics is of great practical significance as a result of toxicity may result from an imbalance between their rates of absorption and elimination. However, the rate of degradation of local anesthetics varies significantly, and this is a vital component in determining the security of a particular agent. For example, in intravenous regional anesthesia of an extremity, about half of the unique anesthetic dose nonetheless is tissue bound 30 min after the restoration of regular blood flow (Arthur, 1987). Reversing the consequences of local anesthetic systemic toxicity is a clinical challenge. Uptake by the lung additionally could play an important function within the distribution of amide-linked native anesthetics. A lidocaine transdermal patch is used for aid of pain related to postherpetic neuralgia. Lidocaine in combination with tetracaine is also provided in a formulation that generates warmth on exposure to air, which is used prior to venous entry and superficial dermatological procedures similar to excision, electrodessication, and shave biopsy of skin lesions. The mild warming is intended to increase skin temperature by up to 5�C for the aim of enhancing supply of local anesthetic into the skin. In addition to preparations for injection, lidocaine is formulated for topical, ophthalmic, mucosal, and transdermal use. In humans, about 75% of the xylidide is excreted within the urine as the additional metabolite 4-hydroxy-2,6-dimethylaniline (Arthur, 1987). Toxicity Local Anesthetics and Related Agents Cocaine Chemistry Cocaine, an ester of benzoic acid and methylecgonine, happens in abundance within the leaves of the coca shrub. The unwanted effects of lidocaine seen with increasing dose embody drowsiness, tinnitus, dysgeusia, dizziness, and twitching. As the dose increases, seizures, coma, and respiratory despair and arrest will occur. The metabolites monoethylglycine xylidide and glycine xylidide could contribute to a few of these unwanted effects. Toxicity and its potential for abuse have steadily decreased the scientific uses of cocaine. Cocaine hydrochloride is offered as a 1%, 4%, or 10% resolution for topical utility. Lidocaine has a wide range of clinical uses as a neighborhood anesthetic; it has utility in nearly any utility where an area anesthetic of intermediate period is needed. Bupivacaine Bupivacaine has a variety of scientific uses as an area anesthetic; it has utility in nearly any software the place a local anesthetic of long length is required. Its lengthy period of motion plus its tendency to present more sensory than motor block has made it a popular drug for providing extended analgesia throughout labor or the postoperative period. Conversely, bupivacaine levels fall extra slowly following cessation of a continuous bupivacaine infusion than can be predicted from single-injection pharmacokinetics. Although lidocaine and bupivacaine each quickly block cardiac Na+ channels throughout systole, bupivacaine dissociates far more slowly than lidocaine throughout diastole, so a big fraction of Na+ channels at physiological coronary heart rates remains blocked with bupivacaine on the end of diastole (Clarkson and Hondeghem, 1985). Thus, the block by bupivacaine is cumulative and substantially greater than predicted by its local anesthetic efficiency. At least a portion of the cardiac toxicity of bupivacaine may be mediated centrally; direct injection of small portions of bupivacaine into the medulla can produce malignant ventricular arrhythmias (Thomas et al. Bupivacaine-induced cardiac toxicity could be tough to treat, and its severity is enhanced by coexisting acidosis, hypercarbia, and hypoxemia, emphasizing the importance of prompt airway management in resuscitation from bupivacaine overdose. The use of prilocaine is essentially limited to dentistry as a outcome of the drug is exclusive among the many local anesthetics in its propensity to trigger methemoglobinemia. Development of methemoglobinemia is dependent on the entire dose administered, usually appearing after a dose of 8 mg/kg.
Chlorophyll. Glucophage SR.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96698
These brokers are used at physiological doses as replacement therapy when endogenous manufacturing is impaired symptoms zinc deficiency glucophage sr 500 mg safe. Glucocorticoids potently suppress inflammation medications contraindicated in pregnancy buy 500mg glucophage sr visa, and their use in inflammatory and autoimmune diseases makes them among the most incessantly prescribed classes of medicine symptoms 0f high blood pressure glucophage sr 500mg purchase on-line. Therefore, the choice to institute remedy with systemic glucocorticoids always requires careful consideration of the relative dangers and advantages in every affected person. Subsequently, Tait and colleagues isolated and characterized a definite corticosteroid, aldosterone, which potently affected fluid and electrolyte balance and therefore was termed a mineralocorticoid. The isolation of distinct corticosteroids that regulated carbohydrate metabolism or fluid and electrolyte steadiness led to the idea that the adrenal cortex comprises two largely unbiased units: an outer zone that produces mineralocorticoids and an inner region that synthesizes glucocorticoids and androgen precursors (reviewed by Miller, 2013). As early as 1912, Cushing described sufferers with hypercorticism, and he later acknowledged that pituitary basophilism triggered the adrenal overactivity, thus establishing the link between the anterior pituitary and adrenal function. The acute part, which happens within seconds to minutes, largely displays an increased supply of ldl cholesterol substrate to the steroidogenic enzymes. The chronic phase, which occurs over hours to days, outcomes largely from increased transcription of the steroidogenic enzymes. To ensure an adequate provide of substrate for steroidogenesis, the adrenal cortex makes use of a quantity of sources of cholesterol, together with circulating ldl cholesterol and cholesterol esters taken up through the low-density lipoprotein and high-density lipoprotein receptor pathways; endogenous cholesterol liberated from cholesterol ester shops through activation of cholesterol esterase; and endogenous ldl cholesterol from de novo biosynthesis. Stress can override the traditional negative-feedback management mechanisms, resulting in marked increases in plasma concentrations of glucocorticoids. Examples of stress indicators embrace injury, hemorrhage, extreme an infection, main surgery, hypoglycemia, cold, pain, and concern. The pathways distinctive to the zona glomerulosa are proven within the orange field; those that happen within the internal zona fasciculata and zona reticularis are shown in the grey box. At the considerably supraphysiological dose of 250 g, cosyntropin maximally stimulates adrenocortical steroidogenesis. An enhance within the circulating cortisol to a degree greater than 18�20 g/dL signifies a traditional response. Cosyntropin may be used diagnostically in adrenal venous sampling to distinguish between unilateral and bilateral aldosterone oversecretion in main aldosteronism. Physiological Functions and Pharmacological Effects Corticosteroids have quite a few effects, which embody alterations in carbohydrate, protein, and lipid metabolism; maintenance of fluid and electrolyte steadiness; and preservation of regular operate of the cardiovascular system, the immune system, the kidney, skeletal muscle, the endocrine system, and the nervous system. In addition, corticosteroids endow the organism with the capability to resist annoying and noxious stimuli and environmental changes. In the absence of enough secretion of corticosteroids from the adrenal cortex, stresses similar to infection, trauma, and extremes in temperature can be deadly. Administration of a small dose of glucocorticoid, however, markedly potentiates the lipolytic motion of these catecholamines. As noted in additional discussion (see structure-activity relationships and Table 46�3), some steroid derivatives present relative selectivity as stimulants of Na+ retention or anti-inflammatory results. Absorption, Fate, and Toxicity Corticotropin is readily absorbed from parenteral websites. Such protein-protein interactions and their consequent negative effects on gene expression seem to contribute significantly to the anti-inflammatory and immunosuppressive results of the glucocorticoids (De Bosscher et al. Aldosterone exerts its results on Na+ and K+ homeostasis primarily through its actions on the principal cells of the distal renal tubules and amassing ducts, whereas effects on H+ secretion largely are exerted within the intercalated cells. In addition to these speedy genomic actions, aldosterone will increase the synthesis of the individual parts of these membrane proteins as part of a more delayed effect. This inactivation allows particular responses to aldosterone in sites such because the distal nephron. In the periphery, glucocorticoids diminish glucose utilization, improve protein breakdown and the synthesis of glutamine, and activate lipolysis, thereby providing amino acids and glycerol for gluconeogenesis. Through their results on glucose metabolism, glucocorticoids can worsen glycemic control in sufferers with overt diabetes and can precipitate the onset of hyperglycemia in prone patients. The second main motion of corticosteroids on the cardiovascular system is to enhance vascular reactivity to different vasoactive substances. The first is the dramatic redistribution of physique fat that occurs in hypercortisolism, such as Cushing syndrome. The other is the permissive facilitation of the lipolytic impact of different brokers, such as growth hormone and adrenergic receptor agonists, leading to an increase in free fatty acids after glucocorticoid administration. Aldosterone is by far essentially the most potent endogenous corticosteroid with respect to fluid and electrolyte steadiness. Thus, the first features of hyperaldosteronism are optimistic Na+ stability with consequent expansion of extracellular fluid volume, normal or slight will increase in plasma Na+ concentration, normal or low plasma K+, and alkalosis. Mineralocorticoid deficiency, in contrast, results in Na+ losing and contraction of the extracellular fluid quantity, hyponatremia, hyperkalemia, and acidosis. Chronically, hyperaldosteronism causes hypertension, whereas aldosterone deficiency can lead to hypotension and vascular collapse. Glucocorticoids also exert effects on fluid and electrolyte balance, largely as a outcome of permissive results on tubular perform and actions that maintain the glomerular filtration price. Excessive quantities of either glucocorticoids or mineralocorticoids also impair muscle perform. This impact, steroid myopathy, accounts partly for weakness and fatigue in patients with glucocorticoid extra. Some sufferers exhibit more pronounced behavioral modifications, corresponding to mania, insomnia, restlessness, and increased motor exercise. A smaller however important percentage of patients handled with glucocorticoids become anxious, depressed, or overtly psychotic. A high incidence of neuroses and psychoses is seen in patients with Cushing syndrome. Addison illness is associated with an elevated mass of lymphoid tissue and lymphocytosis; in contrast, Cushing syndrome is characterised by lymphocytopenia and a decreased mass of lymphoid tissue. A single dose of hydrocortisone leads to a decline of those circulating cells inside 4�6 h; this effect persists for 24 h and results from the redistribution of cells away from the periphery somewhat than from elevated destruction. Finally, glucocorticoids are effective in the treatment of certain lymphoid malignancies, presumably associated to the capability of glucocorticoids to activate apoptosis. Certain water-soluble esters of hydrocortisone and its synthetic congeners are administered intravenously to achieve excessive concentrations of drug quickly in systemic or targeted physique fluids. More prolonged results are obtained by intramuscular injection of suspensions of hydrocortisone, its esters, and congeners. Minor adjustments in chemical structure might markedly alter the rate of absorption, time of onset of impact, and length of action. Glucocorticoids also are absorbed systemically from websites of native administration, similar to synovial areas, the conjunctival sac, skin, and respiratory tract. These effects are important sides of the anti-inflammatory and immunosuppressive actions of the glucocorticoids. Similarly, glucocorticoids are of immense value in treating diseases that end result from undesirable immune reactions. These illnesses range from circumstances that predominantly outcome from humoral immunity, such as urticaria (see Chapter 70), to these which are mediated by mobile immune mechanisms, such as transplantation rejection (see Chapter 35). The immunosuppressive and anti-inflammatory actions of glucocorticoids are inextricably linked, perhaps because they both contain inhibition of leukocyte features. Glucocorticoids inhibit the production by multiple cells of factors that are crucial in generating the inflammatory response. Subsequent reduction of the 3-ketone substituent to the 3-hydroxyl by-product, forming tetrahydrocortisol, happens only within the liver. Such settings embody people with severe hepatic failure and patients with the very uncommon situation of cortisone reductase deficiency. In distinction, aldosterone is exceedingly potent with respect to Na+ retention but has only minimal results on carbohydrate metabolism. A huge array of steroid preparations is on the market for oral, parenteral, and topical use. At doses used for replacement therapy in patients with main adrenal insufficiency, the mineralocorticoid results of these "glucocorticoids" are inadequate to exchange that of probably the most frequent problem in steroid withdrawal is flare-up of the underlying illness for which steroids were prescribed. Protocols for discontinuing corticosteroid therapy in patients receiving long-term remedy have been proposed. These include fluid and electrolyte abnormalities, hypertension, hyperglycemia, increased susceptibility to infection, peptic ulcers, osteoporosis, myopathy, behavioral disturbances, cataracts, progress arrest, and the characteristic habitus of steroid overdose, together with fat redistribution, striae, and ecchymoses. Prudence suggests vigilance for peptic ulcer formation in patients receiving remedy with corticosteroids, particularly if administered concomitantly with aspirin or coxibs.
Nevertheless treatment kidney infection glucophage sr 500mg discount without a prescription, there are pockets of illness around the world medicine in motion quality glucophage sr 500mg, especially in Africa treatment with cold medical term purchase glucophage sr 500mg otc, Asia, and South America. On the other finish of the spectrum is the lepromatous type of the disease (Levis and Ernst, 2005). In some situations, surgical elimination of the infected tissue followed by long-term remedy with effective agents is critical. Acknowledgment: William A, Petri, Jr contributed to this chapter in earlier editions of this book. Drug Facts for Your Personal Formulary: Antimycobacterial Drugs Drug Rifamycins Rifampin � Tuberculosis � M. Treatment and outcome analysis of 205 patients with multidrug-resistant tuberculosis. The Mycobacterium tuberculosis iniA gene is important for activity of an efflux pump that confers drug tolerance to both isoniazid and ethambutol. Isoniazid bactericidal activity and resistance emergence: integrating pharmacodynamics and pharmacogenomics to predict efficacy in different ethnic populations. Cross-resistance between clofazimine and bedaquiline via upregulation of MmpL5 in Mycobacterium tuberculosis. Bactericidal activities of mixtures of new drugs towards Mycobacterium leprae in nude mice. Population pharmacokinetics of rifapentine and its major desacetyl metabolite in South African tuberculosis patients. Overexpression of inhA, but not kasA, confers resistance to isoniazid and ethionamide in Mycobacterium smegmatis, M. Study of efflux pump gene expression in rifampicinmonoresistant Mycobacterium tuberculosis medical isolates. DfrA-thyA double deletion in para-aminosalicylic acid resistant Mycobacterium tuberculosis Beijing. Penetration of rifampicin into the cerebrospinal fluid of adults with uninflamed meninges. Pharmacokinetics and relative bioavailability of clofazimine in relation to food, orange juice and antacid. Meta-analysis of scientific research helps the pharmacokinetic variability hypothesis for acquired drug resistance and failure of antituberculosis remedy. Pharmacokinetics of paraaminosalicylic acid granules underneath 4 dosing conditions. Transfer of embB codon 306 mutations into medical Mycobacterium tuberculosis strains alters susceptibility to ethambutol, isoniazid, and rifampin. The antibiotic resistance arrow of time: 1085 efflux pump induction is a basic first step within the evolution of mycobacterial drug resistance. The molecular foundation of resistance to isoniazid, rifampin, and pyrazinamide in Mycobacterium tuberculosis. Identification of mutations related to streptomycin resistance in medical isolates of Mycobacterium tuberculosis and possible involvement of efflux mechanism. Efflux-pump-derived a number of drug resistance to ethambutol monotherapy in Mycobacterium tuberculosis and the pharmacokinetics and pharmacodynamics of ethambutol. A small-molecule nitroimidazopyran drug candidate for the therapy of tuberculosis. Drug focus thresholds predictive of remedy failure and death in kids with tuberculosis: bread crumb trails in random forests. Population pharmacokinetics of bedaquiline and metabolite M2 in patients with drug-resistant tuberculosis: the impact of time-varying weight and albumin. Ertapenem in the treatment of multidrug-resistant tuberculosis: first medical experience. The antituberculosis drug ethionamide is activated by a flavoprotein monooxygenase. Mutations in panD encoding aspartate decarboxylase are related to pyrazinamide resistance in Mycobacterium tuberculosis. Identification of novel mutations associated with clofazimine resistance in Mycobacterium tuberculosis. Genetic determinants involved in p-aminosalicylic acid resistance in scientific isolates from tuberculosis patients in northern China from 2006 to 2012. Role of acid pH and poor efflux of pyrazinoic acid in distinctive susceptibility of Mycobacterium tuberculosis to pyrazinamide. Nonetheless, fungal infections are associated with significant morbidity and mortality. While amphotericin B remains the gold standard of systemic antifungal pharmacotherapy for a variety of infections, different therapies have emerged for many clinically essential fungal pathogens. This chapter provides a comprehensive overview of at present available therapeutic choices for the management of invasive, mucosal, and superficial fungal infections. Dosing suggestions for antifungal agents in kids have been recently reviewed elsewhere (Autmizguine et al. Polyene macrolide compounds share the traits of 4 to seven conjugated double bonds, an internal cyclic ester, poor aqueous solubility, substantial toxicity when administered systemically, and a standard mechanism of antifungal motion. Amphotericin B is insoluble in water however, when formulated with the bile salt deoxycholate, turns into appropriate for intravenous infusion. Many antifungal brokers act at sites involving cell wall and cell membrane operate. Comparisons Furthermore, the addition of electrolytes to infusion solutions will trigger the colloid to aggregate and complicate administration. Amphotericin B colloidal dispersion accommodates roughly equimolar quantities of amphotericin B and cholesteryl sulfate formulated for injection. The drug is provided as a lyophilized powder and is reconstituted with sterile water for injection (Boswell et al. Antifungal Activity Amphotericin B has helpful medical activity against a broad spectrum of pathogenic fungi, including Candida spp. Fever and headache are widespread reactions that might be decreased by intrathecal administration of 10�15 mg of hydrocortisone. Local injections of amphotericin B into a joint or peritoneal dialysate fluid commonly produce irritation and pain. X-ray crystallography shows the molecule to be inflexible and rod formed, with the hydrophilic hydroxyl groups of the macrolide ring forming an opposing face to the lipophilic polyenic portion. Ergosterol, right here depicted as a green rod, decorates both bilayers of the fungal membrane. Renal tubular acidosis and renal wasting of K+ and Mg2+ also may be seen during and for several weeks after therapy. Anemia is less with lipid formulations and often not seen over the primary 2 weeks. The anemia is more than likely as a outcome of decreased production of erythropoietin and often responds to administration of recombinant erythropoietin. Amphotericin B is also indicated for the therapy of severe or rapidly progressive histoplasmosis, blastomycosis, coccidioidomycosis, and penicilliosis. However, the extra lately developed azoles and echinocandins are usually the medication of alternative for such patients because of their lowered toxicity. Tachypnea, respiratory stridor, or modest hypotension can also happen, however frank bronchospasm and anaphylaxis are uncommon. Patients with preexisting cardiac or pulmonary disease may tolerate the metabolic calls for of the reaction poorly and develop hypoxia or hypotension. The reaction ends spontaneously in 30�45 min; remedy with meperidine may shorten it. The selective action of flucytosine is as a result of of the dearth of cytosine deaminase in mammalian cells, which prevents metabolism to fluorouracil. Approximately 80% of a given dose is excreted unchanged within the urine; concentrations within the urine range from 200 to 500 g/mL. The t1/2 of the drug is 3�6 h in regular individuals and could additionally be as lengthy as 200 h in sufferers with renal failure. Antifungal Activity and Fungal Resistance Flucytosine is presently used primarily as an adjunctive agent with amphotericin B within the induction phase of cryptococcal meningoencephalitis therapy. Imidazoles and triazoles thus impair the biosynthesis of ergosterol, leading to depletion of membrane ergosterol and accumulation of the poisonous product 14-methyl-3,6-diol, resulting in growth arrest (Kanafani and Perfect, 2008), presumably by disrupting the close packing of acyl chains of phospholipids and impairing the features of membrane-bound enzyme systems. Some azoles directly enhance permeability of the fungal cytoplasmic membrane, but the concentrations required are doubtless only obtained with topical use.
A systematic review of aripiprazole-dose treatment for bronchitis order glucophage sr 500mg, plasma focus medicine x topol 2015 cheap glucophage sr 500mg on-line, receptor occupancy ombrello glass treatment cheap 500 mg glucophage sr otc, and response: implications for therapeutic drug monitoring. Augmentation with atypical antipsychotics for melancholy: a review of evidence-based support from the medical literature. This can include prolongation of the inactivated state of voltage-gated Na+ channels, constructive modulation of K+ channels, and inhibition of Ca2+ channels. Much effort is devoted to elucidating the genetic causes and the cellular and molecular mechanisms by which a neural circuit becomes prone to seizure exercise, with the goal of providing molecular targets for both symptomatic and preventive therapies. The term epilepsy refers to a disorder of brain operate characterized by the periodic and unpredictable occurrence of seizures. From a community perspective, seizures arise from cortical, thalamocortical, limbic, or even brainstem circuits. Generalized seizures are actually distinguished by the involvement of the motor system or those who lack motor involvement, for example, typical and atypical absence, eyelid myoclonic. Detailed info pertaining to seizure classifications is presented in Table 17�1. The focal epilepsies could encompass any of the focal seizure varieties (Table 17�1) and account for roughly 60% of all epilepsies. The etiology generally consists of a cortical lesion, such as a tumor, developmental malformation, or harm because of trauma or stroke. The generalized epilepsies are characterized mostly by one or more of the generalized seizure types listed in Table 17�1 and account for about 40% of all epilepsies; the etiology is normally genetic. Focal with Impaired Awareness Focal to Bilateral Tonic-Clonic Impaired consciousness lasting 30 sec to 2 min, typically related to purposeless movements similar to lip smacking or hand wringing. This insightful proposal offered a framework for thinking about mechanisms of focal epilepsy. The pivotal function of synapses in mediating communication amongst neurons in the mammalian brain instructed that defective synaptic function might result in a seizure. That is, a reduction of inhibitory synaptic activity or enhancement of excitatory synaptic activity might be expected to set off a seizure. Glutamate-receptor antagonists also inhibit seizures in various models, together with seizures evoked by electroshock and chemical convulsants. These findings counsel pharmacological regulation of synaptic function can regulate the propensity for seizures and supply a framework for electrophysiological analyses aimed toward elucidating the role of each synaptic and nonsynaptic mechanisms in seizures and epilepsy. However, the placement of the interictal spike helps localize the brain area from which seizure activity originates in a given affected person. Electrographic events with features much like those recorded throughout seizures in vivo have been produced in hippocampal slices by multiple methods, including altering ionic constituents of media bathing the mind slices (McNamara, 1994), such as low Ca2+, zero Mg2+, or elevated K. The accessibility and experimental management supplied by these in vitro 306 preparations has permitted mechanistic investigations into the induction of seizures. Other necessary factors embody the volume of the extracellular house and intrinsic properties of a neuron, similar to voltage-gated ion channels. Identification of these diverse synaptic and nonsynaptic elements controlling seizures in vitro provides potential pharmacological targets for regulating seizure susceptibility in vivo. Effective prophylaxis administered to sufferers at excessive risk would be highly fascinating within the medical setting. Understanding the mechanisms of epileptogenesis in mobile and molecular phrases should present a framework for development of novel therapeutic approaches. Additional models are produced by induction of continuous seizures that final for hours ("status epilepticus"). What transpires through the latent interval between standing epilepticus and emergence of spontaneous seizures that causes the epilepsy Might an antiepileptogenic agent that was efficient in one of these models demonstrate disease-modifying effects in different fashions and maybe in patients The experimental control and accessibility provided by these models-together with careful attention to clinically related concentrations of the drugs-led to clarification of their mechanisms. This sample of neuronal firing is characteristic of a seizure and is unusual during physiological neuronal exercise. Thus, selective inhibition of this sample of firing could be anticipated to reduce seizures with minimal antagonistic results on neurons. Depolarization-triggered opening of the Na+ channels within the axonal membrane of a neuron is required for an action potential. Reducing the speed of restoration of Na+ channels from inactivation may limit the ability of a neuron to fire at high frequencies, an effect that doubtless underlies the effects of carbamazepine, lamotrigine, lacosamide, phenytoin, topiramate, valproate, and zonisamide in opposition to focal seizures. Amongst the various types of generalized seizures, absence seizures have been studied most intensively. The striking synchrony in look of generalized seizure discharges in widespread areas of neocortex led to the concept that a structure in the thalamus or brainstem (the "centrencephalon") synchronized these seizure discharges. Many of the structural and practical properties of the thalamus and neocortex that led to the generalized spike-and-wave discharges have been elucidated (Huguenard and McCormick, 2007). These bilaterally synchronous spike-and-wave discharges, recorded regionally from electrodes in both the thalamus and the neocortex, symbolize oscillations between the thalamus and neocortex. These reverberatory, low-frequency rhythms are made attainable by a mixture of things, including reciprocal excitatory synaptic connections between the neocortex and thalamus in addition to intrinsic properties of neurons within the thalamus (Huguenard and McCormick, 2007). Indeed, bursts of motion potentials in thalamic neurons are mediated by activation of the T-type currents. The inactivated channel itself seems to stay open however is blocked by the inactivation gate, I. Genetics of the Epilepsies Genetic causes contribute to a large variety of human epilepsies. The implication of genes encoding ion channels in familial epilepsy is especially attention-grabbing as a end result of episodic disorders involving different organs additionally end result from mutations of those genes. For instance, episodic issues of the heart (cardiac arrhythmias), skeletal muscle (periodic paralyses), cerebellum (episodic ataxia), vasculature (familial hemiplegic migraine), and different organs all have been linked to mutations in genes encoding components of voltage-gated ion channels (Ptacek and Fu, 2001). However, seizures could come up as a consequence of the cell varieties that express these channels within neural circuits that underlie seizure initiation. Phenobarbital was the first artificial natural agent recognized as having antiseizure activity. Merritt and Putnam developed the electroshock seizure take a look at in experimental animals to display chemical agents for antiseizure effectiveness; in the midst of screening a selection of medicine, they found that diphenylhydantoin (later renamed phenytoin) suppressed seizures in the absence of sedative effects. The maximal electroshock seizure test is extraordinarily priceless as a end result of medicine which would possibly be effective towards the tonic hind limb extension induced by corneal electroshock usually have confirmed to be effective in opposition to focal and generalized tonic-clonic seizures in humans. Parenteral phenytoin is indicated for the management of generalized tonic-clonic standing epilepticus and the remedy of seizures occurring throughout neurosurgery. In poisonous doses, it might produce excitatory signs and at deadly ranges a kind of decerebrate rigidity. Phenytoin limits the repetitive firing of motion potentials evoked by a sustained depolarization of mouse spinal twine neurons maintained in vitro (McLean and Macdonald, 1986a). Once-daily dosing is possible solely with the extended-release formulations, and as a result of differences in dissolution and different formulation-dependent factors, the plasma phenytoin degree could change when changing from one formulation to another. Some agents can compete with phenytoin for binding websites on plasma proteins and enhance free phenytoin at the time the new drug is added to the routine. The plasma t1/2 of phenytoin ranges between 6 and 24 h at plasma concentrations beneath 10 g/mL. At low blood levels, metabolism follows first-order kinetics; as blood ranges rise, the maximal restrict of the liver to metabolize phenytoin is approached, and Cp increases disproportionately as dosage is elevated, even with small changes for levels close to the therapeutic range. Conversely, the degradation price of other medication that serve as substrates for these enzymes may be inhibited by phenytoin; one such drug is warfarin, and addition of phenytoin to a patient receiving warfarin can lead to bleeding problems (Chapter 32). As a general rule, complete control of seizures can be achieved in as much as 50% of sufferers, whereas another 25% could be improved considerably. The degree of success varies as a function of seizure kind, cause, and other factors. Measurement of drug concentrations in plasma facilitates optimizing antiseizure medication, especially when remedy is initiated, after dosage changes, in the event of therapeutic failure, when poisonous results appear, or when multiple-drug therapy is instituted. The final therapeutic routine should be decided by scientific assessment of impact and toxicity. Conversely, the degradation price of other medicine that are substrates for these enzymes may be inhibited by phenytoin. Fosphenytoin is converted into phenytoin by phosphatases in liver and red blood cells with a t1/2 of 8�15 min. Fosphenytoin is extensively sure (95%�99%) to human plasma proteins, primarily albumin. Fosphenytoin is useful for adults with focal or generalized seizures when both intravenous or intramuscular route of administration is indicated.
The kidney treatment 12mm kidney stone glucophage sr 500mg purchase overnight delivery, liver medicine used to treat chlamydia discount glucophage sr 500 mg visa, and spleen also contain high concentrations of colchicine administering medications 7th edition ebook glucophage sr 500mg amex, nevertheless it apparently is basically excluded from heart, skeletal muscle, and brain. Patients with hepatic or renal illness and dialysis patients ought to obtain decreased doses or less-frequent remedy. It is efficient in roughly two-thirds of sufferers if given within 24 h of assault onset. Pain, swelling, and redness abate within 12 h and are fully gone within 48�72 h. The typical dose for prophylaxis in sufferers with normal renal and hepatic perform is zero. Nausea, vomiting, diarrhea, and stomach pain are the most common untoward effects and the earliest indicators of impending colchicine toxicity. During allopurinol treatment, the urinary purines embody hypoxanthine, xanthine, and uric acid. There is a small risk of xanthine stones in patients with a really high urate load earlier than allopurinol therapy, which may be minimized by liberal fluid intake and urinary alkalization. The formation of uric acid stones just about disappears with remedy, which prevents the event of nephropathy. The incidence of acute attacks of gouty arthritis could enhance in the course of the early months of allopurinol therapy as a consequence of mobilization of tissue stores of uric acid. This allows for once-daily dosing and makes allopurinol the most generally used antihyperuricemic agent. Allopurinol and its energetic metabolite oxypurinol are distributed in whole tissue water, with the exception of mind, where their concentrations are about one-third of these in different tissues. Oral therapy provides effective therapy for primary and secondary gout, hyperuricemia secondary to malignancies, and calcium oxalate calculi. The goal of therapy is to cut back the plasma uric acid focus to lower than 6 mg/dL (<360 mol/L) and sometimes lower than 5 mg/dL (<297 mol/L) in patients with tophi to speed up the clearance of monosodium urate. Fluid intake should be enough to keep daily urinary volume larger than 2 L; barely alkaline urine is most well-liked. Those with hematological malignancies may have as a lot as 800 mg/d starting 2�3 days before the start of chemotherapy. Other orphan makes use of for allopurinol include Chagas disease and the ex vivo preservation of cadaveric kidneys prior to transplantation. Thus, when allopurinol is used concomitantly with oral mercaptopurine or azathioprine, dosage of the antineoplastic agent must be reduced to 25%�33% of the usual dose (see Chapters 35 and 66). Although the effect is variable, elevated monitoring of prothrombin activity is really helpful in sufferers receiving each medicines. The concomitant administration of allopurinol and theophylline results in increased accumulation of an lively metabolite of theophylline, 1-methylxanthine; the focus of theophylline in plasma additionally could additionally be increased (see Chapter 40). The cutaneous reaction caused by allopurinol is predominantly a pruritic, erythematous, or maculopapular eruption, but often the lesion is urticarial or purpuric. Because the rash could precede extreme hypersensitivity reactions, patients who develop a rash should discontinue allopurinol. Transient leukopenia or leukocytosis and eosinophilia are rare reactions that may require cessation of therapy. Hepatomegaly and elevated levels of transaminases in plasma and progressive renal insufficiency also could happen. A dose of 40-mg/d febuxostat lowered serum uric acid to comparable levels as 300-mg/d allopurinol. Adverse Events the most typical antagonistic reactions in medical studies had been liver perform abnormalities, nausea, joint ache, and rash. Probenecid 705 Probenecid is a highly lipid-soluble benzoic acid spinoff (pKa three. Thus, febuxostat is contraindicated in patients on azathioprine or mercaptopurine; care must be exercised with concomitant administration of theophylline due to a 400-fold increase within the urinary excretion of the 1-methylxanthine metabolite. The recombinant enzyme, based on the porcine uricase, is administered by infusion. Pegloticase is used for the remedy of extreme, treatment-refractory, persistent gout or when use of other urate-lowering therapies is contraindicated. Rasburicase causes enzymatic degradation of the uric acid in blood samples, and particular handling is required to prevent spuriously low values for plasma uric acid in patients receiving the drug. Uric acid is the one important endogenous compound whose excretion is known to be increased by probenecid. It additionally decreases the biliary secretion of rifampin, leading to higher plasma concentrations. It also is hydroxylated to metabolites that retain their carboxyl function and have uricosuric exercise. Probenecid is marketed for oral administration, alone and together with colchicine. The beginning dose is 250 mg twice daily, increasing over 1�2 weeks to 500�1000 mg twice daily. Higher doses of probenecid (1�2 g/d) are used as an adjuvant to prolong the dwell time of penicillin and other -lactam antibiotics within the body (see Chapter 57). Preparations that combine allopurinol and benzbromarone are more effective than either drug alone in reducing serum uric acid levels, despite the reality that benzbromarone lowers plasma ranges of oxypurinol, the lively metabolite of allopurinol. Renal failure occurred in lower than 1% of patients during combination therapy and approximately 9% during monotherapy. Other antagonistic reactions reported by sufferers during medical trials embody headache (~5%), influenza-like symptoms (~5%), and gastroesophageal reflux (~3%). Acceleration of cardiovascular disease by a dysfunctional prostacyclin receptor mutation: potential implications for cyclooxygenase-2 inhibition. Incidence, presentation, and outcomes in sufferers with drug-induced liver harm in the basic population of Iceland. A perspective on the epidemiology of acetaminophen exposure and toxicity in the United States. Effects of particular inhibition of cyclooxygenase-2 on sodium steadiness, hemodynamics, and vasoactive eicosanoids. Cyclooxygenases, microsomal prostaglandin E synthase-1, and cardiovascular perform. Vascular and higher gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of particular person participant data from randomised trials. Human cyclooxygenase-2 is a sequence homodimer that functions as a conformational heterodimer. Drug resistance and pseudoresistance: an unintended consequence of enteric coating aspirin. Roles of thromboxane A2 and prostacyclin within the development of atherosclerosis in apoE-deficient mice. Differential impairment of aspirin-dependent platelet cyclooxygenase acetylation by nonsteroidal antiinflammatory medicine. Pathogenetic position of cyclooxygenase-2 in hyperprostaglandin E syndrome/antenatal Bartter syndrome: therapeutic use of the cyclooxygenase-2 inhibitor nimesulide. A 4-week, double-blind, parallel-group examine to compare the gastrointestinal effects of meloxicam 7. Nonsteroidal anti-inflammatory medication and hepatic toxicity: a systematic evaluation of randomized controlled trials in arthritis sufferers. Nonsteroidal anti-inflammatory medication and higher and lower gastrointestinal mucosal harm. Nonsteroid drug selectivities for cyclo-oxygenase-1 somewhat than cyclo-oxygenase-2 are associated with human gastrointestinal toxicity: a full in vitro evaluation. Non�mast cell websites of histamine production contribute significantly to the day by day excretion of histamine metabolites within the urine. Because l-histidine decarboxylase is an inducible enzyme, the histamine-forming capacity at such sites is topic to regulation. Distribution and Biosynthesis Distribution Almost all mammalian tissues contain histamine in quantities starting from less than 1 to greater than a hundred g/g. Release and Functions of Endogenous Histamine Histamine is released from storage granules on account of the interplay of antigen with IgE antibodies on the mast cell surface. Histamine performs a central position in quick hypersensitivity and allergic responses. The actions of histamine on bronchial easy muscle and blood vessels account for most of the signs of the allergic response. Histamine is a leukocyte chemoattractant, plays a serious role in regulating gastric acid secretion, and modulates neurotransmitter release.
Because of the affiliation of type 2 diabetes with weight problems within the pediatric age group symptoms 7 days past ovulation purchase 500 mg glucophage sr with mastercard, life-style management is the recommended first step in remedy medicine 91360 purchase glucophage sr 500mg fast delivery. Metformin is approved for children as young as 10 years of age and is available in a liquid formulation (100 mg/mL) georges marvellous medicine cheap 500mg glucophage sr. With chronic administration, circulating insulin levels decline to those that existed before remedy, however regardless of this discount in insulin ranges, reduced plasma glucose levels are maintained. Although their half-lives are brief (3�5 h), their hypoglycemic results are evident for 12�24 h, they usually often may be administered as quickly as day by day. Stress of sickness has been associated with insulin resistance, probably the results of counterregulatory hormone secretion, cytokines, and different inflammatory mediators. Food consumption is commonly variable because of concurrent sickness or preparation for diagnostic testing. Therapy of hyperglycemia in hospitalized patients must be adjusted for these variables. In noncritically unwell hospitalized sufferers, a basal plus bolus correction insulin regimen, adjusted for oral intake, is perfect (Jacobi et al. Intravenous administration of insulin also is properly suited to the therapy of diabetic sufferers through the perioperative period and during childbirth. This may occur because of a change in drug metabolism or extra doubtless from a development of cell failure. Contraindications to using these medication embrace sort 1 diabetes, being pregnant, lactation, and, for the older varieties, important hepatic or renal insufficiency. Rarely, sufferers treated with these medication develop an alcohol-induced flush similar to that caused by disulfiram or hyponatremia. Whether this class of medicine is related to a rise in cardiovascular mortality stays controversial. Some medication (sulfonamides, clofibrate, and salicylates) displace the sulfonylureas from binding proteins, thereby transiently increasing the focus of free drug. Other medication might decrease the glucose-lowering impact of sulfonylureas by rising hepatic metabolism, rising renal excretion, or inhibiting insulin secretion (blockers, Ca2+ channel blockers, cholestyramine, diazoxide, estrogens, hydantoins, isoniazid, nicotinic acid, phenothiazines, rifampin, sympathomimetics, thiazide diuretics, and urinary alkalinizers). Previously out there biguanides, phenformin and buformin, had been removed from the market in the 1970s because of unacceptable charges of associated lactic acidosis. Sulfonylureas similar to glipizide or glimepiride seem safer than longer-acting sulfonylureas in elderly individuals with kind 2 diabetes, but even the short-duration brokers must be used with warning in elderly sufferers. Repaglinide is an oral insulin secretagogue of the meglitinide class (see Table 47�6). Because a small proportion (~10%) is metabolized by the kidney, dosing of the drug in sufferers with renal insufficiency also must be carried out cautiously. Repaglinide also is related to a decline in efficacy (secondary failure) after initially improving glycemic management. Most of the pharmacologic effects of metformin are mediated in the liver with little effect on glucose metabolism or insulin sensitivity in skeletal muscle. Fixed-dose mixtures of metformin along side glipizide, glyburide, pioglitazone, repaglinide, rosiglitazone, linagliptin, saxagliptin, sitagliptin, alogliptin, canagliflozin, dapagliflozin, and empagliflozin are available. A sustained-release preparation is available for once-daily dosing beginning at 500 mg every day, with titration up to 2000 mg as essential. Metformin is effective as monotherapy and in combination with different glucose lowering drugs (Mearns et al. Metformin is mostly accepted because the first-line 876 Metformin has superior or equivalent efficacy of glucose reducing in comparability with other oral agents used to deal with diabetes and reduces microvascular problems in sufferers with type 2 diabetes; more restricted knowledge help a useful effect to cut back macrovascular disease as well. Lactic acidosis related to metformin has been hardly ever reported in sufferers with the setting of concurrent situations that can trigger poor tissue perfusion. It is necessary to assess renal operate before starting metformin and to monitor operate a minimal of annually. Metformin ought to be discontinued preemptively if renal operate may decline precipitously, corresponding to before radiographic procedures that use contrast dyes and during admission to the hospital for extreme sickness. Two thiazolidinediones are presently out there to deal with sufferers with sort 2 diabetes, rosiglitazone and pioglitazone; a third, troglitazone, was faraway from the market in 2000 because of hepatotoxicity. Pioglitazone and rosiglitazone are insulin sensitizers and enhance insulin-mediated glucose uptake by 30%�50% in patients with kind 2 diabetes. Treatment with rosiglitazone or pioglitazone reduces plasma ranges of fatty acids by growing clearance and reducing lipolysis. The onset of action of thiazolidinediones is comparatively slow; maximal effects on glucose homeostasis develop gradually over the course of 1�3 months. The use of insulin with thiazolidinedione therapy roughly doubles the incidence of edema and amount of weight gain in contrast with both drug alone. Macular edema has been reported in sufferers using each rosiglitazone and pioglitazone, but this was not a consistent discovering in current scientific trials (Ambrosius et al. In the past, evidence suggested that rosiglitazone elevated the danger of cardiovascular occasions (myocardial infarction, stroke). The connection of the drug to heart problems remains controversial; most proof supports either gentle beneficial effects of pioglitazone on general cardiovascular occasions or a impartial impression. Therefore, the presence of osteoporosis and other dangers for fracture ought to be thought of before beginning thiazolidinediones. Evidence from medical trials indicated that exenatide can be used at the facet of basal insulin. An extended-release form of exenatide is administered by subcutaneous injection as soon as per week with greater effectiveness than twice-daily treatment. In a single comparative trial, liraglutide lowered A1c about 30% greater than exenatide (Buse et al. Liraglutide is indicated for adjunctive remedy in patients not attaining glycemic management with oral brokers. In a current report, liraglutide decreased the risk of cardiovascular demise, nonfatal myocardial infarction, or nonfatal stroke in patients with sort 2 diabetes and established heart problems. Similar optimistic results on cardiovascular risk have also been demonstrated in a trial of semaglutide, a compound in growth with similarities to liraglutide. Data from a latest medical trial of diabetic subjects with a previous history of cardiovascular disease indicated no impression of lixisenatide on recurrent occasions. Once within the circulation, the drug is metabolized similarly to short-acting exenatide; nevertheless, primarily based on the prolonged price of supply, 5�6 weekly doses are required to reach therapeutic regular state. It is delivered via a pen device at doses of 30 or 50 mg following reconstitution. Clearance of the drug is primarily through enzymatic degradation, though renal clearance may be inferred from the increasing plasma ranges in some patients with renal impairment. Dulaglutide has similar pharmacokinetic properties to albiglutide; no results of hepatic or renal impairment on these has been demonstrated. Lixisenatide has an elimination t1/2 of 3�4 h that includes a major diploma of renal clearance. Clearance of the drug happens primarily by glomerular filtration, with tubular proteolysis and minimal reabsorption. There is a weekly preparation based on the embedding of exenatide in a polymeric microsphere that releases drug slowly after injection. These compounds are also efficient for persistent glucose control when added to the therapy of diabetic patients receiving metformin, thiazolidinediones, sulfonylureas, and insulin, with an extra reduction of A1c by about 0. Acarbose is minimally absorbed; the small quantity of drug reaching the systemic circulation is cleared by the kidney. The -glucosidase inhibitors are contraindicated in patients with stage four renal failure. Alogliptin, saxagliptin, sitagliptin, and vildagliptin flow into primarily in unbound form and are excreted largely unchanged in the urine; decrease doses should be given to patients with reduced renal function. Large cardiovascular safety studies have been completed for alogliptin, saxagliptin, and sitagliptin. Na+-Glucose Transporter 2 Inhibitors Mechanism of Action; Pharmacological Effects. These agents are indicated for use in combination with different oral agents and insulin; such use leads to a further decrease of A1c of zero. Alpha Glucosidase Inhibitors -Glucosidase inhibitors scale back intestinal absorption of starch, dextrin, and disaccharides by inhibiting the action of -glucosidase within the intestinal brush border (Standl and Schnell, 2012). The drugs on this class are acarbose, miglitol, and voglibose (not out there within the U.






