Prozac
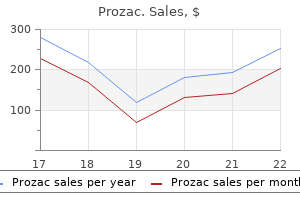
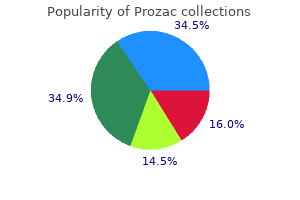
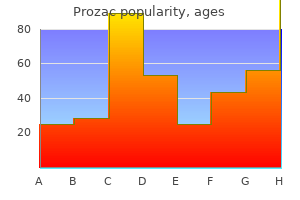
Prozac
Prozac dosages: 20 mg, 10 mg
Prozac packs: 30 pills, 60 pills, 120 pills, 240 pills, 300 pills, 90 pills, 180 pills, 270 pills, 360 pills

Enterobacter bacteremia: scientific options and emergence of antibiotic resistance throughout remedy mood disorder retreats 10mg prozac proven. The relationship between antecedent antibiotic use and resistance to extended-spectrum cephalosporins in group I beta-lactamase-producing organisms depression executive function discount prozac 60 mg on line. Levofloxacin-imipenem mixture prevents the emergence of resistance among clinical isolates of Pseudomonas aeruginosa anxiety medication for children prozac 10mg purchase. Interplay of efflux system, ampC, and oprD expression in carbapenem resistance of Pseudomonas aeruginosa clinical isolates. Pseudomonas aeruginosa ceftolozane-tazobactam resistance development requires multiple mutations resulting in overexpression and structural modification of AmpC. Clinical epidemiology of carbapenem-intermediate or -resistant Enterobacteriaceae. Antibiotic use and the risk of carbapenemresistant extended-spectrum-beta-lactamase-producing Klebsiella pneumoniae infection in hospitalized sufferers: outcomes of a double case-control examine. Antibiotic use and the chance of carbapenemresistant extended-spectrum-beta-lactamase-producing Klebsiella pneumoniae infection in hospitalized patients: results of a double case-control research. Carbapenemase-producing Klebsiella pneumoniae: (when) may we still consider treating with carbapenems Activity of ceftazidime-avibactam towards clinical and isogenic laboratory Pseudomonas aeruginosa isolates expressing mixtures of most relevant beta-lactam resistance mechanisms. Activity of imipenem with relebactam in opposition to gram-negative pathogens from New York City. Antibiotic therapy for Klebsiella pneumoniae bacteremia: implications of manufacturing of extended-spectrum betalactamases. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: our worst nightmare Multidrug efflux pumps and antimicrobial resistance in Pseudomonas aeruginosa and related organisms. Molecular epidemiology and mechanisms of tigecycline resistance in clinical isolates of Acinetobacter baumannii from a Chinese university hospital. Editorial commentary: polymyxin-resistant Acinetobacter baumannii: pressing motion needed. Activity of eravacycline against Enterobacteriaceae and Acinetobacter baumannii, together with multidrug-resistant isolates, from New York City. International convention for the development of consensus on the diagnosis and treatment of ventilator-associated pneumonia. Considerations in control and treatment of nosocomial infections as a end result of multidrug-resistant Acinetobacter baumannii. Antibiotic remedy for Pseudomonas aeruginosa bacteremia: consequence correlations in a potential examine of 200 sufferers. Treatment of pneumococcic meningitis with penicillin in contrast with penicillin plus aureomycin; research together with observations on an obvious antagonism between penicillin and aureomycin. Outcome and attributable mortality in critically unwell patients with bacteremia involving methicillin-susceptible and methicillin-resistant Staphylococcus aureus. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Methicillin-resistant Staphylococcus aureus prolongs intensive care unit keep in ventilator-associated pneumonia, despite initially acceptable antibiotic therapy. Morbidity and cost burden of methicillin-resistant Staphylococcus aureus in early onset ventilator-associated pneumonia. In vitro bactericidal activities of linezolid in combination with vancomycin, gentamicin, ciprofloxacin, fusidic acid, and rifampin against Staphylococcus aureus. In vitro actions of linezolid combined with other antimicrobial agents against Staphylococci, Enterococci, Pneumococci, and selected gram-negative organisms. In vitro exercise of linezolid in combination with doxycycline, fosfomycin, levofloxacin, rifampicin and vancomycin against methicillin-susceptible Staphylococcus aureus. Efficacy of linezolid alone or in combination with vancomycin for remedy of experimental endocarditis because of methicillin-resistant Staphylococcus aureus. Synergy between vancomycin and nafcillin against Staphylococcus aureus in an in vitro pharmacokinetic/pharmacodynamic model. Evaluation of the combination of daptomycin and nafcillin against vancomycin-intermediate Staphylococcus aureus. Clinical practice pointers by the infectious ailments society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and kids. Beta lactam monotherapy versus beta-lactamaminoglycoside mixture therapy for sepsis in immunocompetent sufferers: systematic evaluate and meta-analysis of randomised trials. Treatment of extreme pneumonia in hospitalized sufferers:, outcomes of a multicenter, randomized, double-blind trial evaluating intravenous ciprofloxacin with imipenem-cilastatin. Effect of aminoglycoside and beta-lactam combination remedy versus beta-lactam monotherapy on the emergence of antimicrobial resistance: a meta-analysis of randomized, controlled trials. Potentiation of opsonization and phagocytosis of Streptococcus pyogenes following growth within the presence of clindamycin. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. Impact of antibiotics on expression of virulenceassociated exotoxin genes in methicillin-sensitive and methicillinresistant Staphylococcus aureus. Pathogen- and host-directed anti-inflammatory activities of macrolide antibiotics. Combination antibiotic remedy lowers mortality amongst severely sick sufferers with pneumococcal bacteremia. Lower mortality amongst patients with community-acquired pneumonia handled with a macrolide plus a beta-lactam agent versus a beta-lactam agent alone. Monotherapy versus dual therapy for communityacquired pneumonia in hospitalized patients. Addition of a macrolide to a beta-lactam-based empirical antibiotic regimen is associated with lower in-hospital mortality for sufferers with bacteremic pneumococcal pneumonia. Bacteremic pneumococcal pneumonia in one American city: a 20-year longitudinal examine, 1978-1997. Revisiting combination antibiotic remedy for community-acquired invasive Streptococcus pneumoniae pneumonia. Clinical characteristics at preliminary presentation and impact of dual remedy on the result of bacteremic Streptococcus pneumoniae pneumonia in adults. Penetration of ciprofloxacin in bronchial secretions after intravenous administration. Variability in antibiotic prescribing patterns and outcomes in patients with clinically suspected ventilator-associated pneumonia. Reexamining quinolone use in the intensive care unit: use them right or lose the battle towards resistant micro organism. Impact on the incidence of ventilator-associated pneumonia brought on by antibiotic-resistant gram-negative micro organism. Analysis of vancomycin entry into pulmonary lining fluid by bronchoalveolar lavage in critically unwell patients. Pharmacokinetic and pharmacodynamic profile of linezolid in wholesome volunteers and sufferers with Gram-positive infections. Clinical treatment and survival in Gram-positive ventilator-associated pneumonia: retrospective evaluation of two double-blind research evaluating linezolid with vancomycin. Continuation of a randomized, doubleblind, multicenter study of linezolid versus vancomycin in the treatment of patients with nosocomial pneumonia. Pharmacokinetics and intrapulmonary concentrations of linezolid administered to critically sick sufferers with ventilatorassociated pneumonia. Aerosolized antibiotics for treating hospital-acquired and ventilator-associated pneumonia. Nebulized antibiotics for ventilator-associated pneumonia: a systematic evaluation and meta-analysis. Effectiveness and safety of colistin for the treatment of multidrug-resistant Pseudomonas aeruginosa infections. Utilization of colistin for therapy of multidrugresistant Pseudomonas aeruginosa. Aerosolized plus intravenous colistin versus intravenous colistin alone for the therapy of ventilator-associated pneumonia: a matched case-control examine.
This has but to turn into the standard of care as a result of further study is still required depression help purchase prozac 10mg mastercard. The information for 524 Pa rt 2 Critical Care Cardiovascular Disease perioperative amiodarone use for cardiac surgery are intriguing; nonetheless depression symptoms bereavement prozac 40 mg buy without a prescription, incremental profit beyond -blockade alone has not but been proven anxiety poems 40 mg prozac proven. Prophylaxis against arrhythmia recurrence shares lots of the limitations of acute antiarrhythmic remedy. Digoxin, dofetilide, and sotalol are renally excreted and should be carefully managed (or avoided) to forestall issues in sufferers with renal failure or insufficiency. Amiodarone is hepatically excreted and has the benefit of safety in sufferers with renal insufficiency or renal failure on dialysis. Most digitalis toxicity�related supraventricular arrhythmias result in relatively slow coronary heart rates and are reasonably properly tolerated hemodynamically. A greater share of the speed control group remained on anticoagulation during follow-up. Its major electrophysiologic impact is block of the speedy sodium current responsible for phase zero of the cardiac motion potential. Flecainide has negative inotropic effects associated each to its sodium channel blocking properties and to the reduced drug clearance in sufferers with heart failure. Uncommon noncardiac side effects embrace dizziness, visual disturbances, nausea, and neurologic symptoms. However, not like flecainide it can also block potassium channels, calcium channels, and -adrenergic receptors. Sotalol is run twice day by day at a starting dose of 80 mg and has a half-life of roughly eight hours. In sufferers with a creatinine clearance of 40 to 60 mL/min, the dose should be decreased to once day by day. Food and Drug Administration guidelines, sotalol must be initiated within the hospital with telemetry monitoring. Dofetelide blocks the fast element of the delayed rectifier potassium present, and unlike most other antiarrhythmic medicine it has minimal effects on other ion channels. The starting dose of dofetelide is one hundred twenty five to 500 �g twice daily based on creatinine clearance. It was first developed in the Nineteen Sixties for the treatment of angina, and subsequently within the 1970s, its antiarrhythmic properties were acknowledged. Amiodarone blocks multiple ion channels and subsequently has a extensive range of electrophysiologic results on cardiac tissue. The dose is then lowered to four hundred mg day by day for several weeks and ultimately the maintenance dose is 200 mg day by day. Unfortunately, amiodarone has multiple short-term and long-term side effects that limit its use. Amiodarone contains a big amount of iodine, and is structurally much like thyroid hormone triiodothyronine (T3), and thyroxine (T4). Therefore it inhibits each peripheral conversion of T4 to T3 and entry of T3 and T4 into cells, leading to each hypothyroidism and hyperthyroidism. Pulmonary perform checks present evidence of restrictive physiology and impaired diffusion capacity. Computed tomography scanning of the chest reveals proof of fibrosis and ground-glass opacities. Cutaneous side effects include photosensitivity, and infrequently a blue discoloration of the pores and skin. In the subset of sufferers with ischemic coronary heart disease, amiodarone and sotalol were equally efficacious. Dronedarone has the addition of a methy-sulfonyl group as an alternative of the poisonous iodine moieties, which reduces its interplay with thyroid physiology, decreases its lipophilicity, and shortens its plasma half-life. The most common side effects embody headache, dizziness, nausea, and constipation. Ventricular Arrhythmias the intensivist should be prepared to acknowledge and manage ventricular arrhythmias. Cardiologists and electrophysiologists are sometimes obtainable to assist administration and prescribe long-term treatments. The emergency therapy of cardiac arrest, implantable defibrillators, and pacemakers is covered in Chapters 1 and 5. The first is the presence of two contiguous pathways separated by a central area of inexcitable tissue. Third is a zone of sluggish conduction in one of many pathways to enable restoration and excitation of the area of block, which allows the circuit to perpetuate. Diseased cardiac tissue is especially susceptible to development of enhanced automaticity. Both types of afterdepolarizations happen when oscillations in membrane potential attain the threshold for motion potential formation, leading to abnormal impulse formation. Digitalis inhibitsthesodiumion�potassiumion(Na+-K+) pump, thereby increasingintracellularNa+, which in flip will increase intracellular calcium ion (Ca2+)viatheNa+-Ca2+ exchange present. Movement of intracardiac catheters can end result in mechanically induced arrhythmias. If arrhythmias are thought to be as a end result of catheters, catheter position could also be confirmed by radiography. When it happens in patients with out structural heart illness it typically has a superb prognosis. The enhance in mortality is usually attributed to worsening cardiac illness and not a selected consequence of the shocks. More latest studies, nonetheless, have shown that catheter ablation is most popular over escalation of antiarrhythmic drug remedy. TdP is strongly related to electrolyte abnormalities or medicine that delay repolarization. When this arrhythmia is suspected, a seek for underlying components that can be corrected ought to be undertaken. The ventricular tachycardia on the electrocardiogram appears to rotate round a horizontal axis-hence, the name torsades de pointes, from the French "twisting of the factors. Left ventricular function must be reassessed at forty days after myocardial infarction or 90 days after revascularization. However, it has been proven that serious ventricular arrhythmias not often occur, although the incidence of accelerated idioventricular rhythm may be increased. To ablate it, the decrease third of the septum is mapped to search for the sharpest, earliest Purkinje potential through the tachycardia. Presentation is most common between the ages of 10 and 50 years, with a mean age at diagnosis of approximately 30 years. Note the T-wave inversion in V3 and the unfinished proper bundle branch block pattern. TdP might resolve spontaneously or progress to ventricular fibrillation and cardiac arrest. During electrical storm attributable to Brugada syndrome, isoproterenol infusion may be useful in lessening arrhythmia burden. Shortening of effective refractory intervals combined with increased dispersion of repolarization is the probably substrate for reentry and life-threatening tachyarrhythmias. Males usually have a tendency to be affected and still have an increased risk of sudden dying. Febrile illnesses may set off arrhythmic events in sufferers with Brugada syndrome. The prognosis is poor and effective pharmacologic remedy has not been recognized. Fatal arrhythmias usually have a tendency to be caused by horizontal present circulate (hand to hand); current passing in a vertical style (from head to foot) extra commonly causes myocardial tissue injury. Lightning strike is unique because it causes cardiac and respiratory arrest, resulting in a 25% to 30% mortality price. Electrolyte, Endocrine, and Metabolic Abnormalities Electrolyte and metabolic abnormalities are widespread within the critically sick and should have an result on cardiac depolarization or repolarization.
Too little air flow could be seen as insufficient administration of the very disease being treated anxiety disorder treatment prozac 20 mg buy discount on-line. Current knowledge recommend that the most effective technique is to permit delicate hypercarbia for temporary periods to facilitate decreased air trapping and improved venous return mood disorder or bipolar generic 20mg prozac with visa. In extreme circumstances depression definition weather 40 mg prozac otc, alkalinizing agents may be considered as a further temporizing measure. Peak inspiratory move charges must be set at 60 to eighty L/min with a sq. inspiratory waveform to assist in maximizing expiratory time. In healthy adults, inspiratory:expiratory time ratios are normally 1:2, whereas sufferers with acute bronchial asthma may require ratios of 1:3 to 1:5 or larger. The use of noncompressible tubing additionally facilitates shorter inspiratory and longer expiratory occasions. Alternative and Investigational Agents New medications and old medications with traditionally nonasthma indications are postulated to have potential utility in the treatment of bronchial asthma every day. Such agents which have demonstrated early or intermittent promise include methotrexate, antifungal agents, macrolide antibiotics, ketamine, inhaled heparin, furosemide, and anesthetics. However, this therapy remains invasive and controversial and consideration for its use should be reserved for those with acceptable experience and experience. Heavy sedation with or with out paralysis reduces carbon dioxide manufacturing, facilitates correct measurement of airway pressures, and reduces dyssynchrony and discomfort. Strategies to facilitate correct delivery include doubling doses and inserting the nebulization system as close to the patient as attainable. If tidal volumes are shallow (<7 mL/ kg), inspiratory pressure can be increased steadily by 2 cm H2O every 15 minutes to a objective to scale back the respiratory fee to less than 25 breaths/min87�93 (also see Chapter 10). Obesity within the United States has reached epidemic ranges and its impact on new adult-onset bronchial asthma and the severity of the disease is well known. Concomitant mental sickness and gastroesophageal reflux illness have been demonstrated to worsen asthmatic signs and to make control tougher. In addition to other risk factors, such as prior hospitalizations and intubations, gastroesophageal reflux illness and psychological illness were related to elevated utilization of well being care sources and increased 30-day readmission charges. Examples embody bronchial asthma education, follow-up cellphone calls, help and facilitation of primary and specialist follow-up appointments, and extra. Gibeon and colleagues developed 11 bronchial asthma facilities across the United Kingdom that used standardized remedy approaches and reported right into a national database. This intervention decreased steroid use and improved quality-of-life scores however, again, the influence on life-threatening asthma stays unknown. Bryant-Stephens and colleagues made residence visits and located high-risk dwellings with mite and cockroach infestations, mold, overcrowding, and persistent exposure to tobacco smoke and unhealthy diets. Investigators partnered with New York housing administration to identify at-risk sufferers and to optimize alternatives to maximize modification of risk-dwelling updates and discount of onsite triggers as examples. Most studies concentrate on the collective muscle weakness and polyneuropathies that happen because of their use, notably at the aspect of corticosteroids, heavy sedation, and the critical care surroundings. Such neuromuscular derangements are more prevalent in females with renal failure and hypophosphatemia. Steroid myopathy, against this, primarily entails proximal muscle tissue and the creatine kinase levels are usually normal. In the rare affected person who must be repeatedly paralyzed, infusions must be stopped each 4 to 6 hours to decrease dosing and accumulation and to facilitate neurologic evaluation. A peripheral nerve stimulator must be used to limit paralysis to at least a recording of one or two twitches in response to a train-of-four stimulus. Life-threatening bronchial asthma in adult patients is more frequent in those with earlier critical exacerbations, those that are female, overweight, and African American. Corticosteroids and inhaled bronchodilators stay the cornerstones of rescue therapy, and invasive mechanical ventilation may be required for those with refractory airflow obstruction. Immune-modulating medication are more and more acknowledged as potential adjunctive or replacement brokers. Efforts to modify risk factors such as obesity, psychological sickness, and comorbidities and efforts to maximize illness administration and avoidance of triggers proceed to be fundamental to the success of asthma care and the avoidance of life-threatening episodes. Key Points � the prevalence of bronchial asthma in the United States continues to steadily decrease and mortality is highest in African American girls older than sixty five years of age. What is the evidence for harm of neuromuscular blockade and corticosteroid use in the intensive care unit Lack of therapeutic profit and increase of the toxicity from aminophylline given in addition to high doses of salbutamol delivered by metered-dose inhale with a spacer. Heliox-driven 2-agonist nebulization for kids and adults with acute asthma: a systematic review with meta-analysis. Nebulized versus intravenous albuterol in hypercapnic acute asthma: a multicenter, double-blind, randomized study. Rates and characteristics of intensive care unit admissions and intubations amongst asthma-related hospitalizations. Management based on global initiative for bronchial asthma tips of patients with near-fatal asthma reduces morbidity and mortality. Trends in asthma prevalence, health care use, and mortality within the United States, 2001�2010. The impact of volume infusion on dead space in mechanically ventilated patients with extreme asthma. Acute bronchial bronchial asthma: relations between scientific and physiologic manifestations. Continuous intravenous terbutaline infusions for adult patients with standing asthmaticus. Factors for poor prognosis of near-fatal bronchial asthma after restoration from a life threatening bronchial asthma assault. Comparison of the effect on blood gases, air flow, and perfusion of isoproterenol-phenylephrine and salbutamol aerosols in persistent bronchitis with asthma. American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Effects of short-term 28% and one hundred pc oxygen on arterial carbon dioxide rigidity and peak expiratory circulate price in acute athma: a randomized trial. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma: Update on Selected Topics 2002. High serum albuterol ranges and tachycardia in adult asthmatics treated with high-dose repeatedly aerosolized albuterol. Management of acute bronchial asthma in adults in the emergency department: assisted air flow. Cost-benefit comparison of aerosol bronchodilator supply strategies in hospitalized patients. Comparison of the cardiopulmonary effects of subcutaneously administered epinephrine and terbutaline in patients with reversible airway obstruction. Combined inhaled beta-agonist and anticholinergic agents for emergency administration in adults with asthma. Nebulized salbutamol with and without ipratropium bromide in acute airflow obstruction. Use of heliox in sufferers with extreme exacerbation of continual obstructive pulmonary disease. Heliox-driven beta2-agonist nebulization for youngsters and adults with acute bronchial asthma: a systematic review with meta-analysis. Effect of heliox- and air-driven nebulized bronchodilator remedy on lung function in patients with bronchial asthma. Does aminophylline profit adults admitted to the hospital for an acute exacerbation of bronchial asthma Intravenous aminophylline confers no extra benefit in acute asthma treated with intravenous steroids and inhaled bronchodilators. Treatment of acute asthma: lack of therapeutic profit and enhance of the toxicity from aminophylline given along with high doses of salbutamol delivered by metered-dose inhaler. Magnesium sulfate for treating exacerbations of acute extreme asthma in the emergency department. Omalizumab for the remedy of severe persistent allergic asthma: a systematic evaluation and economic analysis. Omalizumab remedy for adults and kids with allergic asthma: a evaluation of the scientific effectiveness, cost-effectiveness, and tips. Efficacy and security of a recombinant anti-immunoglobulin E antibody in extreme allergic bronchial asthma. Pharmacokinetics, pharmacodynamics and clinical efficacy of omalizumab for the therapy of bronchial asthma.
Ventricular fibrillation in hypercalcaemic disaster because of anxiety over ebola prozac 40mg generic free shipping main hyperparathyroidism baseline depression definition prozac 10 mg buy low cost. Calcium free hemodialysis: expertise in the remedy of 33 patients with severe hypercalcemia depression symptoms severe 40 mg prozac generic mastercard. Zoledronic acid is superior to pamidronate within the treatment of hypercalcemia of malignancy: a pooled evaluation of two randomized, controlled medical trials. Physiological and pathophysiological function of magnesium in the cardiovascular system: implications in hypertension. Effects of dietary vitamin D on magnesium absorption and bone mineral contents in pigs on normal magnesium intakes. Hypomagnesemia in critically ill cancer sufferers: a prospective examine of predictive factors. Proton pump inhibitors and hypomagnesemia in the basic inhabitants: a population-based cohort study. Proton-pump inhibitor-induced hypomagnesemia: Current analysis and proposed mechanisms. High incidence of hypophosphatemia in surgical intensive care patients: efficacy of phosphorus therapy on myocardial operate. Pathophysiologic and medical correlates of hypophosphatemia and the connection with sepsis and consequence in postoperative sufferers after hepatectomy. Hypophosphatemia induced by mechanical air flow in sufferers with chronic obstructive pulmonary disease. Severe hypophosphatemia during hematopoietic reconstitution after allogeneic peripheral blood stem cell transplantation. A new graduated dosing regimen for phosphorus replacement in sufferers receiving diet assist. Fatal hyperphosphatemia following Fleet Phospho-Soda in a patient with colonic ileus. Hyperphosphatemic hypocalcemic coma attributable to hypertonic sodium phosphate (fleet) enema intoxication. Spurious hyperphosphatemia because of sample contamination with heparinized saline from an indwelling catheter. Metastatic calcification of the cardiac conduction system with heart block: an under-reported entity in chronic renal failure patients. Which of the following statements concerning the therapy of lactic acidosis with sodium bicarbonate is most correct Treatment of lactic acidosis with sodium bicarbonate will trigger a rise in carbon dioxide generation, which can lower intracellular pH. By raising extracellular pH, bicarbonate administration will scale back ionized calcium (answer a incorrect). By inflicting systemic alkalinization, bicarbonate administration is likely to trigger a rise in lactate generation fee (answer d incorrect). The affected person was admitted with sepsis from a urinary supply and has been intubated and receiving pressors (norepinephrine and dopamine) for the previous three days. On examination his very important indicators are within normal limits and he appears to be comfortable and in no distress. Urinary electrolytes embody the following: urinary sodium 87 mEq/L, urinary potassium 35 mEq/L, and urinary chloride a hundred and ten mEq/L. Which of the following is the more than likely rationalization for the elevated potassium stage There are numerous causes for hyperkalemia in critically unwell patients, together with extreme potassium load, translocation of potassium throughout mobile membrane, and lack of ability to get rid of excess balance. Pseudohyperkalemia is the more than likely clarification due to normal laboratory findings the day before without change in clinical status. Pseudohyperkalemia has several attainable causes, together with hemolysis and fist clenching with a tourniquet in place throughout phlebotomy (answer d correct). A 3% sodium chloride (NaCl) infusion is started at eighty mL/h and after 6 hours the sodium degree is 122 mmol/L. Stop the 3% NaCl, start 5% dextrose in water (D5W) and desmopressin to lower the sodium stage. Patients with acute symptomatic hyponatremia have to be treated with an infusion of 3% saline answer to rapidly enhance the plasma sodium focus and prevent cerebral edema. The sodium aim is 6 mmol/L in the first 24 hours as a more rapid rise is pointless and can induce osmotic demyelination syndrome. This patient had a really speedy enhance in the sodium degree; therefore, the sodium concentration should be lowered. Monitoring chemistry (choice a), administration of normal saline solution (answer b) may lead to even more rapid increase in sodium. Zoledronic acid Answer four: a Treatment of hypercalcemia consists of calcium elimination and decreased bone resorption. Zoledronic acid is among the most efficacious bisphosphonates used to treat hypercalcemia (answer d incorrect). Calcitonin rapidly reduces calcium ranges but its effects dissipate inside 72 hours (answer b incorrect). Hemodialysis can be utilized in sure instances to deal with refractory hypercalcemia (answer c). Despite its impact on calcium degree, the use of plicamycin is discouraged because of its side effect profile (renal liver and bone marrow toxicity) (answer a correct). The anion gap is the difference between measurements of positively charged and negatively charged particles. Initial plasma laboratory findings are as follows: sodium 130 mmol/L, potassium three. He is intubated and treatment with intravenous regular saline resolution containing dextrose, thiamine, and folic acid is started. Which of the following electrolyte disturbances would the affected person be on the highest danger of growing with the described treatment This patient has threat components and bodily findings of long-standing malnutrition and is at threat of creating the refeeding syndrome as a result of endogenous insulin secretion in response to dextrose. Hypernatremia is unlikely to develop with isotonic fluids (answer a incorrect), and insulin-mediated potassium entry into cells would most probably result in hypokalemia quite than hyperkalemia (answer b incorrect). Hypermagnesemia would doubtless not happen without excessive magnesium ingestion (answer c incorrect), and because the metabolic acidosis (likely ketoacidosis) corrects, the blood pH will rise, thus putting him in danger for hypocalcemia owing to displacement of albuminbound protons with calcium (answer d incorrect). As the -cell production of insulin falls, glucose ranges additional improve, exacerbating the method. In the absence of insulin the liver, adipose tissue, and skeletal muscle are unable to use glucose and sense a state of "hunger. Osmolality can be calculated using glucose and sodium: [2(measured Na) + glucose/18]. Dextrose is added to the fluids as quickly as the plasma glucose degree falls beneath 200 to 250 mg/dL. When the plasma glucose degree falls below 200 to 250 mg/ dL, the infusion rate must be decreased to zero. Check capillary glucose and serum/urine ketones to verify hyperglycemia and ketonemia/ketonuria. Keep serum glucose between 200 and 300 mg/dL till patient is mentally alert K+ = three. Notes: 15 to 20 mL/kg/hour; serum Na must be corrected for hyperglycemia (for every one hundred mg/dL glucose, add 1. In sufferers not beforehand utilizing insulin, the subcutaneous insulin dose must be extrapolated from the final 6 to eight hours of the insulin infusion rate. It is essential that the patient is at a gentle state and not taking pressors earlier than making this estimation. To discover the total every day dose of insulin, the imply insulin rate is multiplied by 20 to enable for a 20% reduction in the calculated dose. Potassium Serum potassium concentration is usually elevated on account of extracellular shift of potassium. Hypotension, energetic sepsis, use of pressors, and intubation are contraindications to transition as a result of these factors are acknowledged to be associated with unreliable subcutaneous insulin absorption, with continued want for probably the most versatile dosing because of incessantly changing insulin necessities. Bridge over troubled waters: safe and effective transitions of the inpatient with hyperglycemia.
Risk of acute kidney damage in sufferers on concomitant vancomycin and piperacillin-tazobactam in comparability with bipolar depression medication and weight loss 20 mg prozac discount with mastercard those on vancomycin and cefepime anxiety lightheadedness 10mg prozac cheap with mastercard. Systematic evaluate and metaanalysis of acute kidney harm related to concomitant vancomycin and piperacillin/tazobactam mood disorder nos code buy discount prozac 10mg on line. Initiation of inappropriate antimicrobial remedy leads to a fivefold discount of survival in human septic shock. Inadequate antimicrobial treatment: an essential determinant of consequence for hospitalized patients. The effect of pathophysiology on pharmacokinetics in the critically sick patient�concepts appraised by the instance of antimicrobial agents. Clinical importance of delays within the initiation of acceptable antibiotic therapy for ventilator-associated pneumonia. Community-acquired bacterial meningitis: threat stratification for opposed medical consequence and effect of antibiotic timing. Surviving sepsis marketing campaign: international tips, for administration of severe sepsis and septic shock: 2008. Pharmacodynamic properties of antibiotics: utility to drug monitoring and dosage regimen design. Piperacillin penetration into tissue of critically unwell sufferers with sepsis�bolus versus continuous administration Therapeutic drug monitoring of beta-lactams in critically sick patients: proof of concept. Insufficient beta-lactam concentrations within the early part of severe sepsis and septic shock. Continuous infusion of beta-lactam antibiotics in severe sepsis: a multicenter double-blind, randomized managed trial. Experience with a once-daily aminoglycoside program administered to 2,184 adult sufferers. Evaluation of intravenous ciprofloxacin in patients with nosocomial decrease respiratory tract infections. Impact of plasma concentrations, organism, minimal inhibitory concentration, and scientific situation on bacterial eradication. The disaster of resistance: identifying drug exposures to suppress amplification of resistant mutant subpopulations. Augmented renal clearance: implications for antibacterial dosing in the critically unwell. Assessment of renal perform in scientific follow at the bedside of burn patients. Accuracy of short-duration creatinine clearance determinations in predicting 24-hour creatinine clearance in critically ill and injured sufferers. Pharmacodynamics and pharmacokinetics of antibacterial medicine in the management of febrile neutropenia. A comparison of estimates of glomerular filtration in critically ill sufferers with augmented renal clearance. Sub-therapeutic initial beta-lactam concentrations in select critically unwell patients: affiliation between augmented renal clearance and low trough drug concentrations. Augmented renal clearance in septic patients and implications for vancomycin optimisation. Flucloxacillin dosing in critically unwell patients with hypoalbuminaemia: special emphasis on unbound pharmacokinetics. The effects of hypoalbuminaemia on optimizing antibacterial dosing in critically sick patients. Resolution of infectious parameters after antimicrobial remedy in sufferers with ventilator-associated pneumonia. Experience with a medical guideline for the therapy of ventilator-associated pneumonia. International scientific practice tips for the treatment of acute uncomplicated cystitis and pyelonephritis in girls: a 2010 replace by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Efficacy and security of procalcitonin guidance in decreasing the length of antibiotic treatment in critically sick sufferers: a randomised, controlled, open-label trial. For optimum clinical consequence when selecting empiric antimicrobial therapy, which of the next decisions is correct The clinician should adjust antimicrobial remedy on day 2 or 3 of the medical course. Empiric therapy should be sufficient not only for the correct antibiotic based mostly on susceptibility of the organism but in addition for optimum dose/ dose interval, right route of administration, and use of combination remedy if needed. Other variables playing a role in optimal medical end result embody time of administration and pharmacologic properties of the agent. Another level to consider is the potential for choice of antibiotic resistance. Which one of the following antibiotics would be effective in treating an an infection attributable to an extended-spectrum lactamase�producing strain of Klebsiella species Even antibiotics which may be stable in the presence of -lactamases could not have a predictable activity. The knowledge extrapolated from medical literature recommend that carbapenems are the drug of choice to deal with such infections. Which antibiotic ought to be prevented while treating an Enterobacter an infection if laboratory knowledge suggest susceptibility The most frequently cited effect is synergy, which has been well described with penicillin and ampicillin with gentamicin in treatment of enteroccocal endocarditis. In the intensive care unit an important benefit of using mixture therapy is that it increases the prospect of sufficient remedy when dealing with multidrug-resistant organisms. Increasing populations of immunocompromised hosts with serious fungal and viral infections usually require critical care, and sufferers hospitalized in critical care models are also susceptible to these infections. Effective administration of these circumstances not solely requires use of the appropriate anti-infective agents, but in-depth information of their pharmacodynamic/pharmacokinetic properties, as well as awareness of their physiologic results, toxicities, and drug interactions. Recent years have also introduced important antifungal and antiviral drug developments, giving the clinician an ever-increasing arsenal of therapeutic decisions. The involved reader is referred to the Infectious Diseases Society of America pointers on the topic. Both drugs have essential toxic results that often restrict their use in patients with organ/system failure. Topical remedy of candidiasis and therapy of other systemic fungal infections are omitted or solely briefly Amphotericin B and Its Lipid Formulations Amphotericin B is produced by Streptomyces nodosus and is considered one of the oldest and most generally used antifungal agents. Once within the bloodstream, it dissociates and binds to plasma proteins and lipoproteins. First, a really acute type of renal dysfunction appears to be related to amphotericin B�induced renal arteriolar constriction. The renal harm also reduces erythropoietin production15 and thus causes a gentle anemia throughout chronic remedy (the hematocrit typically falls to about 30%). Finally, amphotericin B may precipitate cardiac arrhythmias, especially if the affected person is already hypokalemic and hypomagnesemic. To avoid producing a precipitate, it must be diluted in an electrolyte-free solution at no more than zero. It should be administered over a minimal of 1 hour and most authorities favor a 2- to 3-hour infusion. Premedication with acetaminophen, diphenhydramine, and steroids could also be used if the patient develops reactions to the infusion. Volume loading appears to cut back nephrotoxicity, and many authorities give (if possible) 500 to one thousand mL regular saline answer simply before each dose of amphotericin B. Administration via a central line is advisable as peripherally given amphotericin B usually produces phlebitis. Treatment targets have been traditionally and arbitrarily cumulative (such as 1 or 2 whole g), however a time-based approach is increasingly used for some ailments. A typical dose is 50 mg of amphotericin B diluted in a thousand mL of water and irrigated over 24 hours. A small number of intracranial fungal infections profit from intrathecal dosing at zero. Intraperitoneal amphotericin B is contraindicated, as it may trigger excruciating ache and peritoneal fibrosis. The optimum dose of those compounds is unclear and the brokers seem usually equipotent. Dosages of ~3 mg/kg per day would appear suitable for remedy of most severe Candida infections.
Taxus brevifolia (Yew). Prozac.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96779
Diagnosis of ventilatorassociated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic "blind" bronchoalveolar lavage fluid depression symptoms loneliness generic prozac 40 mg. Clinical prognosis of ventilator related pneumonia revisited: comparative validation utilizing immediate postmortem lung biopsies anxiety and nausea prozac 60 mg purchase with visa. Reintubation increases the risk of nosocomial pneumonia in sufferers needing mechanical air flow postnatal depression definition nhs 40mg prozac discount. Colonization of dental plaque: a source of nosocomial infections in intensive care unit sufferers. Aspiration of gastric micro organism in antacid-treated patients: a frequent cause of postoperative colonisation of the airway. The effect of stress ulcer prevention on the incidence of pneumonia in artificial respiration. A comparison of sucralfate and ranitidine for the prevention of higher gastrointestinal bleeding in patients requiring mechanical ventilation. Impact of allogenic packed purple blood cell transfusion on nosocomial infection charges within the critically unwell patient. Association of noninvasive air flow with nosocomial infections and survival in critically sick sufferers. Effect on the length of mechanical ventilation of figuring out sufferers able to breathing spontaneously. Protocol-driven ventilator weaning reduces use of mechanical air flow, price of early reintubation, and ventilator-associated pneumonia. Improving adherence to a mechanical ventilation weaning protocol for critically ill adults: outcomes after an implementation program. Daily sedation interruption versus no daily sedation interruption for critically sick grownup sufferers requiring invasive mechanical air flow. Effect of protocolized sedation on scientific outcomes in mechanically ventilated intensive care unit patients: a scientific review and meta-analysis of randomized managed trials. Early tracheostomy for primary airway administration in the surgical important care setting. The impact of a complete oral care protocol on sufferers at risk for ventilator-associated pneumonia. Continuous aspiration of subglottic secretions in stopping ventilator-associated pneumonia. A randomized medical trial of continuous aspiration of subglottic secretions in cardiac surgical procedure sufferers. A potential, randomized comparability of an in-line warmth moisture trade filter and heated wire humidifiers: rates of ventilator-associated early-onset (communityacquired) or late-onset (hospital-acquired) pneumonia and incidence of endotracheal tube occlusion. Influence of airway management on ventilator-associated pneumonia: evidence from randomized trials. A randomized medical trial comparing an extended-use hygroscopic condenser humidifier with heated-water humidification in mechanically ventilated patients. Prevention of ventilator-associated pneumonia: an evidence-based systematic evaluate. The Trach Care closed tracheal suction system: a brand new medical system to permit tracheal suctioning with out 484. Incidence of colonization, nosocomial pneumonia, and mortality in critically sick patients using a Trach Care closed-suction system versus an open-suction system: prospective, randomized study. Nosocomial pneumonia in mechanically ventilated sufferers, a prospective randomised analysis of the Stericath closed suctioning system. Mechanical air flow with or with out daily adjustments of in-line suction catheters. Nosocomial pneumonia in ventilated trauma patients throughout stress ulcer prophylaxis with sucralfate, antacid, and ranitidine. Selective decontamination of the digestive tract and ventilator-associated pneumonia (part 1). Selective decontamination of the digestive tract and ventilator-associated pneumonia (Part 2). Selective digestive tract decontamination-will it prevent an infection with multidrug-resistant gram-negative pathogens however nonetheless be applicable in establishments where methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci are endemic The direct costs of nosocomial catheter-associated urinary tract an infection in the period of managed care. A potential study of pathogenesis of catheter-associated urinary tract infections. Systematic evaluate: antimicrobial urinary catheters to stop catheter-associated urinary tract an infection in hospitalized sufferers. A prospective, randomized, investigator-blinded trial of a novel nitrofurazone-impregnated urinary catheter. Efficacy of antimicrobialimpregnated bladder catheters in decreasing catheter-associated bacteriuria: a prospective, randomized, multicenter scientific trial. The efficacy of silver alloy-coated urinary catheters in preventing urinary tract infection: a meta-analysis. Risk components for fluoroquinolone resistance in nosocomial Escherichia coli and Klebsiella pneumoniae infections. Epidemiological investigation of fluoroquinolone resistance in infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Academic detailing to enhance use of broad-spectrum antibiotics at a tutorial medical center. Decrease in nosocomial Clostridium difficile�associated diarrhea by proscribing clindamycin use. Manipulation of a hospital antimicrobial formulary to control an outbreak of vancomycinresistant enterococci. Changes within the prevalence of vancomycin-resistant enterococci in response to antimicrobial formulary interventions: impression of progressive restrictions on use of vancomycin and third-generation cephalosporins. A hospitalwide intervention program to optimize the standard of antibiotic use: impression on prescribing follow, antibiotic consumption, price financial savings, and bacterial resistance. Cycling empirical antimicrobial agents to stop emergence of antimicrobial-resistant gram-negative micro organism amongst intensive care unit patients. The impression of an antibiotic biking program on empirical remedy for gram-negative infections. Minimizing antimicrobial resistance in hospital micro organism: can switching or cycling medicine assist Providing appropriate antimicrobial remedy within the intensive care unit: surveillance vs. Antibiotic use and microbial resistance in intensive care units: impression of computer-assisted choice support. Selective decontamination of the digestive tract in the intensive care unit: present status and future prospects. Effect of selective decontamination of the digestive tract on respiratory tract infections and mortality within the intensive care unit. Meta-analysis of randomised managed trials of selective decontamination of the digestive tract. Prophylaxis with enteral antibiotics in ventilated patients: selective decontamination or selective cross-infection Effectiveness of antibiotic prophylaxis in critically unwell grownup patients: systematic review of randomised managed trials. Selective decontamination of the digestive tract in surgical sufferers: a systematic review of the proof. The role of selective digestive decontamination for reducing an infection in sufferers present process liver transplantation: a systematic evaluation and meta-analysis. Impact of selective decontamination of the digestive tract on fungal carriage and an infection: systematic evaluation of randomized controlled trials. Selective decontamination of the digestive tract reduces bacterial bloodstream infection and mortality in critically ill sufferers. Antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults receiving intensive care. Changing bacterial ecology during a five-year interval of selective intestinal decontamination.
Syndromes
The attributable morbidity and mortality of ventilator-associated pneumonia within the critically unwell affected person mood disorder blogs 10 mg prozac cheap overnight delivery. Mortality rate attributable to ventilatorassociated nosocomial pneumonia in an grownup intensive care unit: a prospective case-control research depression retreat buy prozac 10mg with mastercard. Outcome and attributable value of ventilator-associated pneumonia amongst intensive care unit patients in a suburban medical heart depression symptoms after a death prozac 60mg buy overnight delivery. Attributable price of catheter-associated bloodstream infections amongst intensive care patients in a nonteaching hospital. A decade of decreased gram-negative infections and mortality associated with improved isolation of burned sufferers. Antimicrobial stewardship programs have been shown to enhance an infection cure charges, scale back therapy failures, increase frequency of correct antibiotic prescribing, and reduce antibiotic resistance and C. Prolonged use of broad-spectrum antimicrobial therapy is associated with antimicrobial resistance and C. Antibiotic stewardship is outlined as coordinated interventions designed to enhance the appropriate use of antibiotic agents by promoting the choice of the optimum antibiotic drug routine together with dosing, period of remedy, and route of administration. Antibiotic stewardship programs have been proven to enhance infection treatment rates, cut back treatment failures, improve frequency of correct antibiotic prescribing, and decrease antibiotic resistance and C. Prospective audits with intervention and feedback and formulary restriction and preauthorization are core methods of antimicrobial stewardship programs. The highest charges of bloodstream infections are seen with the use of hemodialysis catheter (10% of patients). Arterial catheters have rates of device-related bloodstream an infection in the range of solely 1%. Central vein catheters in the subclavian vein or internal jugular have rates of device-related bloodstream infections in the vary of 3% to 5%. Swan-Ganz pulmonary artery catheter use is related to a 1% to 3% danger of bloodstream infections. Infection rates are associated with the usage of correct sterile approach at insertion time. Use standard precautions, including the usage of gloves and robe as applicable, during any manipulation of catheter or collecting system d. Maintaining a closed drainage system is essential; if a break in aseptic technique, disconnection, or leakage happens, exchange the catheter and accumulating system. Use of ordinary precautions, together with the usage of gloves and robe as acceptable, throughout any manipulation of the catheter or accumulating system is really helpful. It is recommended to maintain an unobstructed urine flow, including maintaining the amassing bag below the level of bladder always, maintaining the catheter and accumulating tube free from kinking, and emptying the collecting bag regularly. Other sources exist exogenously, corresponding to bacteria dropped at patients from inadequately washed arms, inadequately disinfected respiratory remedy equipment, contaminated medicine vials, and inadequately disinfected nebulizers shared amongst patients. A 40-year-old male with a historical past of alcoholism and injection drug use presents heavily intoxicated and requires intubation for airway protection. On day three of mechanical ventilation he develops fever, leukocytosis, new lung infiltrates as seen on chest x-ray, and increased tracheal secretions. The American Thoracic Society and Society of Critical Care Medicine recommends an invasive diagnostic method similar to bronchoalveolar lavage as it has been proven to decrease mortality. The microbial spectrum shifts to nosocomial brokers the longer affected person is supported by mechanical air flow and is uncovered to antibiotics. Often, the newer drug may have more efficiency, a extra fascinating dosing schedule, or a better side effect profile. The usual state of affairs is that the "old" drug nonetheless works, however the "new" ones work higher. Indeed, the issue is in many ways self-inflicted, attributable to misuse and overuse of antimicrobials. In the crucial care setting, antibiotic choice usually entails a two-stage process: empiric therapy, adopted by de-escalation to directed, definitive therapy upon identification of the pathogen. Four focuses of antibiotic prescribing are of main importance in each the scientific and public well being context: the proper drug, the proper time, the right dose, and the best length. Practitioners must combine antibiotics with an infection prevention for it to be optimally effective. Awareness of such components is important within the development of the knowledge base relating to sufficient antibiotic remedy and its effect on not solely morbidity and mortality but in addition the hospital ecology. Appropriate empiric therapy � Influenced by surveillance information providing prevalence of resistant pathogens and by local antibiograms giving susceptibility knowledge � Consideration of mixture therapy to cowl more than likely pathogens, including those with antibiotic resistance 2. Utilization of antibiotic pharmacodynamics/ pharmacokinetics and properties � Dosing patterns � Dosing changes based on clearance 2. Role of mixture therapy � Antibiotic synergy versus antagonism � Antibiotic indifference however improved clinical efficacy three. Several ideas influence antibiotic prescription for an individual affected person, first in empiric after which in directed remedy. Antibiotic selection always happens inside the context of the entire intensive care unit, raising ideas related to antibiotic stewardship that may conflict or compete with those influencing antibiotic prescription. Individually, none of those trials reported important variations in clinical response or mortality rates between comparator arms with the exceptions of tigecycline5 and doripenem,6 which had been both associated with worse outcomes. In the absence of definitive knowledge from the trials, the authors carried out a series of meta-analyses evaluating each class of antibiotics towards all other classes to decide whether any class of antibiotics might be superior to another. Several variables affect decisions about number of the "right drug," including the microbiology of antibiotic-resistant organisms and the pharmacology of the antimicrobial agents used to deal with infections. A fundamental understanding of the mechanisms of resistance and the organisms that specific them can lead to more practical empiric therapy and a extra efficient de-escalation course of. When these two parameters have been used in subcategories to evaluate the predisposition for selecting resistant organisms, antibiotic use was a more influential issue than was mechanical air flow. The problem for the clinician is to achieve the appropriate degree of steadiness between these two opposing results. Research has shown that intermittent antibiotic exposures lead quickly to the evolution of tolerance-the ability to survive under therapy with out creating resistance. Using in vitro evolution experiments, investigators have proven that tolerance usually precedes resistance, with mathematical inhabitants genetics modeling exhibiting that tolerance boosts the probabilities for resistance mutations to spread in the inhabitants. Such information supplies perception into the impression of antimicrobial publicity on bacterial ecology. Clinical implications of this embrace the importance of minimizing pointless broadness and length of antibiotic remedy. Clinical Responses to Multidrug Resistance Antibiotic resistance results in delays in appropriate antibiotic remedy and subsequent treatment failure. To attain its target site, an antibiotic must penetrate the outermost a part of the bacterial cell wall; thus impermeability precludes the drug from attending to its target website. Once an antibiotic enters the bacterial cell wall, but earlier than it binds to its target site, there are two potential mechanisms by which the bacteria can prevent the antibiotic from reaching its effect: (1) enzymatic destruction of the antibiotic and (2) extrusion of the drug from the micro organism by way of efflux pumps. Because of the significance of enzymatic destruction and of efflux that results in the drug resistance encountered in the crucial care setting, these two mechanisms of motion are mentioned in some element; nonetheless, it is important to think about the importance of target-site binding and of impaired penetration because each mechanisms of resistance have practical implications for the clinician. The medical significance of this mechanism is finest represented by a comparatively frequent practice. An uninformed follow sample is the addition of a -lactamase inhibitor like clavulanic acid to a drug like amoxicillin as the subsequent agent used in an attempt to treat that infection. Binding to a Target Site Penetration Through the Bacterial Cell Wall An antibiotic should penetrate the bacterial cell wall to attain its goal binding site. Normally a point of entry for nutrients into the micro organism and excretory products out of the micro organism, antibiotics, most notably carbapenems, use porin channels as the route of entry. The most important instance of resistance mediated by porin channel closure is the resistance of Pseudomonas aeruginosa to carbapenems. Enzymatic degradation of antibiotics is among the most widespread and variable mechanisms of antibiotic resistance out there to microorganisms. The basic example of resistance by enzymatic destruction is the cleaving-and subsequent inactivation-of -lactam antibiotics by the -lactamase family of enzymes. Because countless -lactamase enzymes exist, clinicians should use a clinically related classification system. The Ambler classification divides -lactamase enzymes into 4 distinct lessons.
Although clonic motor activity in these patients remains seen postpartum depression definition who buy 20 mg prozac visa, it may be difficult to decide whether or not a subsequent further decline in alertness displays a seizure or some other course of lithium depression definition prozac 60mg buy cheap on line. Thus any affected person who manifests these findings and who has a possible reason for seizures anxiety self test order prozac 20 mg with mastercard. Many kinds of irregular movements happen in patients with extreme metabolic disturbances or anoxic mind harm. During therapeutic cooling for sufferers in a coma after cardiac arrest, seizures could additionally be troublesome to detect clinically, especially when neuromuscular junction blockade is used. Consciousness is immediately lost, and after several seconds the tonic section offers method to clonic (rhythmic) extension of the extremities, with flexion occurring during each brief rest. Although clonic motor activity is the most easily acknowledged form, the seizure will take on the functional characteristics of the adjacent practical tissue. This may, unfortunately, result in both diagnostic obscuration and iatrogenic problems. Beyond trying to defend the affected person from hurt, very little may be done with enough rapidity to affect the course of the seizure. This is the most effective time to collect evidence of a focal onset, which means structural mind illness. The postictal examination is equally priceless; language, motor, sensory, or reflex abnormalities after an apparently generalized convulsion also wants to be viewed as evidence of focal illness. A full listing of doubtless epileptogenic medication is past the scope of this chapter; the drugs of any patient who has a seizures must be reviewed with this possibility in thoughts. Although ethanol withdrawal is the most typical offender, discontinuing any hypnosedative agent. The physical examination ought to be carried out with particular emphasis on the factors mentioned earlier for the postictal examination. In addition, evidence of cardiovascular disease (as a source for cerebral emboli) and systemic an infection must be sought. In addition to routine biochemical studies, screening for medication of abuse must be performed on sufferers with unexplained seizures. Cocaine has emerged as a prominent explanation for seizures in many city hospitals44 and newer proconvulsant synthetic substances should nonetheless be suspected within the presence of unfavorable results of a toxicology screen. Hyperparathyroidism has been linked anecdotally to seizures, with the inference that parathormone is neurotoxic. Similarly, hypomagnesemia has an unwarranted reputation as a cause of seizures, especially within the malnourished alcoholic patient. In specific, stages of the electrographic development may be sufficiently brief to be ignored. Partially treating status epilepticus might dissociate the scientific and electrographic options. The preliminary high-frequency discharge turns into progressively less well shaped over minutes; this sample implies that neuronal activity is much less synchronous. Such a affected person may have prophylaxis against delirium tremens with benzodiazepines, however the seizures themselves seldom require treatment. It is now obvious that initiating antiseizure drug therapy after the primary unprovoked. Although the same old objective of continual antiseizure drug remedy is to administer the smallest dose of a tolerated single agent that utterly controls seizures, such an method is often inconceivable within the important care environment. Calculations of the unbound focus based on the serum albumin concentration are unreliable. Hepatic dysfunction will mandate a decrease in the upkeep dose; if the serum albumin is very low, the loading dose can be lowered as well. This allergy may be manifested solely as fever, however more generally it features a rash and eosinophilia. The first panel illustrates the onset of the seizure; the following panels present its evolution. Montage: longitudinal bipolar; channels 1 to four, left temporal; and channels 5 to eight, left parasagittal. Valproate must be averted in settings in which liver disease or hyperammonemia could additionally be problematic however is otherwise a useful drug available each orally and intravenously. A loading dose of 30 mg/kg is cheap, followed by a maintenance dose of 30 to 60 mg/kg per day. The usual dose for seizure prevention is between 500 and 1500 mg/day, though doses up to 6 g/day have been used. Lacosamide is also available intravenously and is started at a dose of 200 mg twice daily. Thus upkeep doses of this agent need be given solely once a day, and a steady-state degree will take about 3 weeks to be established. Oral loading with carbamazepine in conscious sufferers might produce coma lasting a number of days. It should be recalled as a cause of hyponatremia in sufferers receiving it chronically. In a patient with any of those circumstances, the clinician should transfer shortly to cease seizures to stop additional mind destruction. If endotracheal intubation underneath neuromuscular junction blockade is critical, use a nondepolarizing agent. If increased intracranial stress is a concern, premedicate with lidocaine (1 mg/kg). If the affected person is hypotensive, start quantity substitute and/or vasoactive agents as clinically indicated. Unless the patient is known to be normoglycemic or hyperglycemic, administer dextrose (1 mg/kg) and thiamine (1 mg/kg). Propofol 50�250 �g/kg per min loading dose adopted by a maintenance infusion at a price of 5�60 �g/kg per min 3. Pentobarbital 12-mg/kg loading dose followed by a upkeep infusion at a price of 0. Higher doses of those sedative brokers may be needed in sure clinical conditions. With any breakthrough seizure requiring uptitration of sedative drips, second-line antiseizure drug therapeutic levels must be maximized or another antiseizure drug must be added. Slow sedative taper must be initiated as soon as the patient is seizure-free for greater than 24 h. In these uncommon circumstances, initiation of any of the following fourth line therapies is really helpful: 1. Ketamine 1- to 5-mg/kg loading dose (may repeat every 5 min as a lot as three times) adopted by a maintenance infusion at a fee of 1. Addition of different nonconventional antiseizure medication (topiramate, clonazepam, clobazam, vigabatrin) three. Rhabdomyolysis should be treated with a vigorous saline answer diuresis to forestall acute renal failure; urinary alkalinization may be a useful adjunct. In rare cases, cool peritoneal lavage or extracorporeal blood cooling could additionally be required. Its main advantage is a very lengthy length of motion as soon as an enough dose has been administered (the 20-mg/kg loading dose reliably produces a complete serum focus above 20 �g/mL for 24 hours). The drug can even cause thrombophlebitis, which can end result in the "purple glove syndrome. The maximal recommended price of infusion is a hundred and fifty mg/min, nevertheless it must be began extra slowly and elevated to this fee if tolerated. Although these agents are efficient if utilized in large sufficient doses, unwanted side effects typically restrict their use64 or could even be deadly. It has been successful in case series66,67 however has not been instantly compared to the opposite available brokers. Up to 37% of those patients are actually recognized to have an autoimmune or paraneoplastic cause for his or her condition. Although these conditions of patients generally seem hopeless, it may be very important remember that 35% will return to their premorbid degree of operate. Expert opinion is split relating to the probably epileptic nature of those phenomena. Another area of contention concerns the epileptiform discharges regularly seen after respiratory or cardiac arrests. This effect on prognosis appeared to be due to the effect of the reason for the ictus, rather than the seizure itself. Other causes related to marked will increase in mortality fee have been anoxia, intracranial hemorrhages, tumors, infections, and trauma.
These modifications create the ideal electrophysiologic and anatomic substrate for creating reentrant arrhythmias anxiety zantac prozac 60 mg generic free shipping. This research was designed to examine the efficacy of moricizine depression zone buy cheap prozac 60 mg online, flecainide mood disorder lupus buy cheap prozac 20mg on line, or encainide in patients after a myocardial infarction with decreased ejection fractions and frequent ventricular ectopic beats. Although flecainide was efficient in suppressing ventricular ectopy, there was a threefold improve in arrhythmic deaths compared with placebo. Specific Clinical Considerations Hypertensive Encephalopathy Hypertensive Crisis in Cerebrovascular Accidents Acute Aortic Dissection Hypertensive Crises in Pregnancy Postoperative Hypertension Catecholamine-Associated Hypertensive Crisis Conclusions Introduction and Terminology Hypertension is a standard medical disorder and one of the most widespread preventable contributors to disease and death. However, a small subset can expertise vital acute end-organ damage and these sufferers require immediate remedy to stop irreversible organ dysfunction. The report of the Eighth Joint National Committee on EvidenceBased Guidelines for the Management of High Blood Pressure in Adults defines hypertension as a systolic pressure of a hundred and forty mm Hg or higher and/or a diastolic stress of 90 mm Hg or larger. For instance, an acute increase in diastolic blood strain to a price of one hundred mm Hg may cause important damage in a previously normotensive particular person, whereas a diastolic pressure of a hundred thirty mm Hg may be tolerated in a patient with a historical past of uncontrolled hypertension. A hypertensive emergency is a severe elevation in blood pressure related to the presence of acute end-organ harm. Hypertensive emergencies require quick control of blood strain, inside 1 to 2 hours to stop additional organ injury. The absolute stage of blood stress and the time course of this elevation determine the development of a hypertensive emergency. However, acute end-organ injury can occur at totally different blood strain values in numerous sufferers. Depending on the inhabitants studied, 20% to 50% of patients presenting with a hypertensive emergency have a secondary cause of hypertension recognized. These elevations of blood pressure can be related to persistent steady organ dysfunction, such as stable angina, chronic renal insufficiency, or earlier cerebrovascular accident, with out proof of acute endorgan damage. Organ ischemia will increase launch of vasoconstrictors, and a vicious circle is initiated. Pathophysiology the underlying pathophysiology of hypertensive crises is still not fully understood. The transition of mild hypertension or normotension to a hypertensive crisis is normally attributable to an occasion that results in an abrupt increase in blood pressure. Situations related to this occasion may embrace cessation of hypertensive medications with potential rebound effects, consumption of illicit medication, and extreme ache, in addition to several medical syndromes. In most hypertensive crises, the initial rise in blood stress is secondary to increased systemic vascular resistance. The rise in systemic vascular resistance is believed to be brought on by humoral vasoconstrictors. However, a scientific method with consideration of underlying pathophysiology may help the clinician to keep away from widespread pitfalls within the clinical management of patients with hypertensive crises. The commonest pitfall in treating patients with hypertensive crises includes treating numbers with out evaluating particular person patients for acute end-organ damage. A methodical approach to patients with severe elevations in blood stress can help set up safe and effective therapy. In sufferers with hypertensive emergencies (the presence of acute end-organ damage), the blood stress must be lowered acutely to a protected goal to forestall additional end-organ damage. A centered history ought to decide a previous analysis of hypertension, medication historical past, use of illicit drugs or over-the-counter brokers with potential hypertensive results, and the presence of signs according to neurologic, visible, cardiac, or renal dysfunction. It is necessary to measure blood pressure adequately and in each upper extremities. Pulses should also be checked in all extremities, as inequalities in blood pressure or pulses can exist with aortic dissection. In addition, a radical neurologic and cardiopulmonary examination ought to consider possible indicators of end-organ failure such as altered mentation, new focal neurologic deficits, or cardiogenic pulmonary edema. A funduscopic examination of the eyes should be done to search for signs of acute papillary edema or new retinal hemorrhages. A set of straightforward diagnostic exams can full the analysis for acute end-organ damage. Abnormalities in blood urea nitrogen, creatinine, and the urinalysis (red blood cell casts) recommend renal involvement. Additional exams could also be indicated primarily based on the individual traits of each case. However, if after a careful systematic scientific evaluation, Does this affected person have psychological status change It is necessary to emphasize that the presence or absence of acute end-organ damage and never the numerical value of the blood pressure ought to dictate the acuity with which blood stress reduction should be achieved. The targets for treating hypertensive emergencies are to lower blood pressure to a stage that forestalls ongoing acute end-organ harm and at the similar time to avoid iatrogenic harm caused by precipitous falls in blood strain causing hypoperfusion to organs. Understanding the autoregulation of blood strain in regular states and in patients with persistent hypertension is important to obtain these targets. With chronic hypertension, compensatory useful and structural modifications occur within the vasculature. Hence, patients with continual hypertension have a better tolerance to elevated blood pressures, as their autoregulatory curve is shifted to the best. This explains why many sufferers current with severely elevated blood stress and no evidence of acute end-organ harm. However, rapid reductions of blood stress to "normal" levels can fall under the lower autoregulatory capacity of the circulation in a chronically hypertensive affected person. Systematic evaluation for potential acute end-organ harm can proceed based on this scheme. If the reply to any of the questions is "Yes," the patient has a hypertensive emergency and blood strain ought to be lowered acutely. Cerebral blood flow autoregulation curves are depicted for normotensive (solid purple line) and persistent hypertensive (dashed blue line) states. The perfect medicine to treat a hypertensive emergency should have a speedy onset of action, high efficiency, instant reversibility, no tachyphylaxis, and minimal or no adverse effects. There are a restricted number of research evaluating agents by way of scientific outcomes. With no clear outcome information, the choice of an agent is predicated on the clinical situation, pharmacologic traits of the drug, and availability. Parenteral brokers that are helpful in treating hypertensive emergencies are further discussed (in alphabetical order). Clevidipine has vasoselective properties with a fast onset of action and a very quick half-life (<1 minute). Clevidipine reduces blood pressure by a direct and selective effect on arterioles. The initial dose is often 1 to 2 mg/h with adjustments as needed to obtain the desired response in blood stress. The upkeep dose is normally four to 6 mg/h; however, larger doses could additionally be required in certain scientific conditions. Small studies have in contrast clevidipine to nitroprusside for the treatment of extreme hypertension in anesthetized sufferers present process surgical procedure. Although clevidipine has not been studied extensively in other clinical situations, its traits make it a beautiful choice for the remedy of hypertensive emergencies outdoors the operating room. In addition to its intraoperative use it has received increased consideration in neurologic hypertensive emergencies. Esmolol Esmolol is an ultra�short-acting cardioselective, -adrenergic agent that might be administered intravenously for the remedy of hypertensive emergencies. An different regimen is a continuous infusion starting at 1 to 2 mg/min and titrated upward to obtain a desired blood strain endpoint. Adverse effects of labetalol embody orthostatic hypotension, bronchospasm (should be prevented in asthma patients), coronary heart failure, and vital bradycardia (should be averted within the presence of sinus bradycardia or heart block greater than first degree). Labetalol has been proven to be efficient in a wide range of medical situations associated with hypertensive emergencies. Labetalol lowers blood stress by decreasing systemic vascular resistance by 1-blockade and on the similar time counteracts the reflex tachycardia from vasodilation via its -blocker effect.






