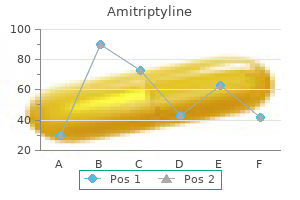
Amitriptyline
Amitriptyline
Amitriptyline dosages: 50 mg, 25 mg
Amitriptyline packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Instillation of anesthetic gel into the urethra has not been found to be of serious profit in ladies depression symptoms negative thoughts amitriptyline 50 mg buy otc, most likely due to the straighter urethra (Patel et al depression fallout 50 mg amitriptyline visa. Aspiration with use of a 60-mL syringe connected to the irrigant port is often essential through the process depression symptoms graves disease 25 mg amitriptyline generic otc. The use of air cystoscopy, as opposed to fluid instillation, has additionally been evaluated and located to potentially assist in visualization during energetic hematuria (Ciudin et al. Attempts have been made to modify the beforehand described surveillance schedule with use of decision evaluation instruments (Abel, 1993; Kent et al. Several authors suggest termination of surveillance at 5 or more years for low-risk sufferers (Haukaas et al. However, the precise cost of surveillance cystoscopy was liable for solely 13% of the expenditures for bladder most cancers care in a single study, so the financial alternative may be restricted for such efforts (Hedelin et al. In addition, the risk of recurrence and potential for development exists beyond this period. Other investigators have examined the predictive impact of early or multiple recurrences and how this may have an result on surveillance (Holm�ng et al. Tumor recurrence on initial 3-month cystoscopy and variety of tumors on preliminary resection (single or multiple) provide probably the most predictive data with regard to recurrence in several studies. Absence of recurrence on the 3-month surveillance cystoscopy in patients with Ta low-grade tumors is associated with recurrence rates so low that annual cystoscopy appears safe even at that point (beginning 12 months after the preliminary resection) (Fitzpatrick et al. Urine Cytology Cytology involves microscopic evaluation of stained cellular smears from the urine. Its high specificity is crucial function of cytology as a outcome of a constructive reading regardless of cystoscopic or radiographic findings suggests the existence of malignancy within the overwhelming majority of sufferers. Although cytology has traditionally been believed to have high sensitivity for high-grade cancer, current research counsel that only 58% of bladder tumors are recognized utilizing cytology. Cumulative information from sequence revealed after 1990 reported that cytology actually recognized (using the older grading system) 11% of grade 1, 31% of grade 2, and solely 60% of grade three tumors (Halling et al. In distinction, they observed that these current findings were well under those reported earlier than 1990, when the sensitivity of cytology was 94% for grade 3 tumors, but may discover no explanation for this deterioration. These findings are supported by numerous different research and emphasised by a latest multicenter study involving several establishments noted for bladder cancer expertise that discovered cytology had an overall sensitivity of 15. Benign conditions of the urinary tract corresponding to stones, an infection, inflammation, hematuria, and cystoscopy can cause a false-positive reading. A laboratory-based, quantitative immunoassay and a qualitative point-of-care test can be found. Sensitivities were 50% and 90% for noninvasive and invasive cancer, respectively, with an general sensitivity of 55. Probes to determine aneuploidy of chromosomes 3, 7, and 17 are combined with a probe to the 9p21 locus. Probes may be developed to determine essentially any locus, but this mix has the most effective sensitivity and specificity (Halling et al. It will, however, detect chromosomal modifications earlier than the development of phenotypic expression of malignancy, so it leads to an "anticipatory optimistic" studying in some sufferers. Most of these have had adequate sensitivity however poor specificity, resulting in substantial false-positive readings, creating the need for further diagnostic testing. Current urinary markers have been developed to detect tumorassociated antigens, blood group antigens, development factors, cell cycle and apoptosis, and extracellular matrix proteins. The most vital issue limiting widespread adoption of tumor markers is the lack of potential data to assist their influence on prognosis or illness management (Lokeshwar et al. The general sensitivity of these exams ranges from 50% to 80%, whereas the specificity is between 50% and 75%. These checks are extra delicate than cytology notably for low-grade tumors, but their results can be falsely constructive in patients with irritation, infection, or hematuria (Liou, 2006). ImmunoCyt (DiagnoCure, Saint Foy, Canada) is a hybrid of cytology and an immunofluorescence assay. The assay has not been shown to be affected by benign conditions, but interpretation is complicated and operator dependent (T�tu et al. This test could additionally be helpful in adjudicating atypical cytology as a result of it has a high negative predictive value on this setting (Odisho et al. An irregular enlarged cell (lower right) demonstrates three copies of chromosome three (red), chromosome 7 (green), and chromosome 17 (aqua) on use of fluorescence in situ hybridization. Magnetic resonance urography and renal ultrasound are potential alternate options in select patients. Although rare, the appearance of upper tract illness is related to mortality charges of 40% to 70%. The risk for recurrence in this population appears biggest over the primary 5 years after remedy (median time to detection, fifty six months) but persists a minimal of 15 years. Involvement of the ducts by high-grade disease is finest managed by radical cystoprostatectomy, and consideration of urethrectomy must be made, especially if tumor is present near or on the surgical margin (Liedberg et al. In abstract, surveillance methods ought to be individualized on the idea of the danger of recurrence within the bladder and extravesical sites (see Table 136. Moreover, patients testing negative are unlikely to expertise tumor recurrence in less than 1 yr (Yoder et al. UroVysion has additionally been shown to make clear equivocal findings in patients with atypical or unfavorable cytology (Skacel et al. CxBladder Monitor is a noninvasive urine monitoring test using gene expression and medical affected person knowledge to generate a take a look at to assess for proof of urothelial carcinoma. A retrospective examine suggests that a multiplex of eight biomarkers in combination might enhance efficiency compared with presently out there markers if validated in further research (Rosser et al. For instance, if indication for biopsy within the operating room is the top point, then excessive specificity is desired to restrict the number of unfavorable biopsies. On the other hand, if increasing the interval of cystoscopic surveillance is the top level, then excessive sensitivity, significantly for high-grade tumors, is desired. Defining that a affected person has a low likelihood of recurrence within the following year can enable individualization of surveillance protocols (see Table 136. They do, however, counsel consideration of urinary markers to assess response to intravesical therapy in addition to for the adjudication of atypical or equivocal cytology outcomes (Chang et al. Secondary Prevention Strategies Lifestyle changes and chemoprevention may potentially reduce the danger of recurrence and have been thought of within the management of patients with non�muscle-invasive illness. Smoking cessation, increased fluid intake, and a low-fat diet could cut back the risk of recurrence; the former is paramount. Increased hydration reduces the focus and dwell time of carcinogens and thereby reduces the danger of malignant transformation within the urothelium (Jiang et al. Isoflavones have been studied for a similar function, however the studies have been abandoned because of larger bladder most cancers danger within the sufferers consuming greater amounts of soy products (Sun et al. Synchronous tumors have been detected in no sufferers (0) with grade 1 (using the prior grading system) tumors, 1. In a evaluation of 591 sufferers with median follow-up of 86 months, higher tract recurrence was zero. In the setting of intermediate- or high-risk patients, guidelines suggest consideration of surveillance upper tract imaging at 1- to 2-year intervals, but there are few data evaluating the good factor about such imaging (Chang et al. Thesurveillance schedule should be individualized on the premise of danger stratification of essentially the most lately resected tumor. Aldousari S, Kassouf W: Update on the administration of non-muscle invasive bladder most cancers, Can Urol Assoc J 4(1):56�64, 2010. Amling C, Thraser J, Frazier H, et al: Radical cystectomy for stages Ta, Tis, and T1 transitional cell carcinoma of the bladder, J Urol 151:31, 1994. Anderson C, Weber R, Patel D, et al: A 10-item checklist improves reporting of critical procedural elements during transurethral resection of bladder tumor, J Urol 196:1014�1020, 2016. Azuma T, Nagase Y, Oshi M: Pyuria predicts poor prognosis in patients with non�muscle-invasive bladder most cancers, Clin Genitourin Cancer 11(3):331�336, 2013. Bassi P, Spinadin R, Carando R, et al: Modified induction course: an answer to side-effects Berrum-Svennung I, Granfors T, Jahnson S, et al: A single instillation of epirubicin after transurethral resection of bladder tumors prevents only small recurrences, J Urol 179(1):101�105, 2008.
Cells mature from the basal basement membrane cells depression economic definition purchase 50 mg amitriptyline amex, that are small and cuboidal anxiety tips amitriptyline 50 mg buy lowest price, to intermediate cells to superficial umbrella cells in an orderly fashion anxiety prescriptions purchase amitriptyline 50 mg online. The floor has massive umbrella cells which will have nuclear atypia and kind asymmetrical items. These umbrella cells type a urine bladder barrier preventing toxins from reworking urothelial cells. Precursor lesions are a continuum from hyperplasia to atypia to dysplasia and eventually cancer. Although the nuclei may be slightly enlarged, no cytologic atypia is current and mitoses are absent. On cystoscopy, papillary urothelial hyperplasia can be indistinguishable from low-grade papillary lesions and is commonly present adjacent to low-grade papillary tumors. Reactive atypia is characterized by nuclear abnormalities occurring in the background of an infected urothelium (Hodges et al. Typically sufferers have a history of chronic irritation, regeneration, or reaction from noxious stimuli and have irritative voiding symptoms. Microscopically, although nuclei may be distinguished and enlarged, the mucosa proceeds in an orderly fashion from basal to intermediate to superficial cell sorts, and nuclear polarity is maintained. Urothelial dysplasia is characterized by a normal urothelial thickness and an altered cytologic look of urothelial cells. Normal cytoplasmic clearing is lost notably in basal and intermediate cells, with lack of nuclear polarity, nuclear enlargement, hyperchromosia, and nuclear membrane irregularity. The lamina propria is typically regular, and comparison with normal urothelium might help differentiate reactive atypia from dysplasia. Malignant Lesions Urothelial carcinoma is the most typical malignancy of the urinary tract and is the second most typical reason for demise among all genitourinary tumors. There is severe nuclear atypia, lack of cellular polarity, and a non-cohesive mobile construction. The cells are giant, pleomorphic, chromatin clumping, and infrequently with abnormal mitotic figures. Low-grade Ta tumors frequently recur 48% to 71% of the time; however, stage or grade progression is relatively rare, occurring 2% to 12% of the time, relying on the sequence (Montironi and Lopez-Beltran, 2005). There is a disordered progress pattern, numerous mitotic figures current, and there are pleomorphic cells with exaggerated nuclei. If left untreated, more than 80% of high-grade papillary tumors invade the underlying urothelial stroma. High-grade papillary tumors are thought of biologically, and clinically, to be a precursor to invasive high-grade urothelial cancer. These stratifications suggest that the deeper the tumor invades into the lamina propria, the extra severe the survival. T2a includes invasion into the internal half of the muscularis propria, though T2b is deeper into the outer half. T3 illness constitutes invasion outdoors of the bladder proper into the periadipose tissue. T4a illness is invasion of the prostatic stroma, uterus, or vagina, and T4b illness is invasion of the pelvic or stomach wall. Prostatic urethral cancer is associated with bladder most cancers in 90% of instances, although amongst sufferers with major bladder urothelial most cancers, urethral involvement is comparatively uncommon, occurring in 3% of sufferers. Prostate stromal invasion, however, notably whether it is direct extension from the bladder by way of the muscle into the prostate, does carry a poor prognosis, with 5-year total survival of less than 25% in historic collection (Donat et al. For this reason only patients with prostate stromal invasion are thought-about to be T4. Molecular Biology Major progress has been made in recent years towards bettering our understanding of the molecular make-up of urothelial carcinoma. It has grown towards the hollow center of the bladder however has not grown into the connective tissue or muscle of the bladder wall. It has not grown inward toward the hollow part of the bladder, nor has it invaded the connective tissue or muscle of the bladder wall. The cancer has grown into the layer of connective tissue under the lining layer of the bladder but has not reached the layer of muscle in the bladder wall (T1). The cancer has grown into the internal (T2a) or outer (T2b) muscle layer of the bladder wall, however it has not passed utterly via the muscle to reach the layer of fatty tissue that surrounds the bladder. The most cancers has grown by way of the muscle layer of the bladder and into the layer of fatty tissue that surrounds the bladder (T3a or T3b). The most cancers has grown via the bladder wall into the pelvic or stomach wall (T4b). The cancer might or may not have grown through the wall of the bladder into nearby organs (Any T). It has spread to 1 or extra distant organs (such because the bones, liver or lungs) (M1b). Ras genes are from a household of transforming oncogenes that have been originally identified in T24 bladder cancer cell lines (McBride et al. A new framework is emerging for understanding the heterogeneity of bladder cancer and the way that molecular diversity performs a role in treatment response. In the first pathway, tumors arise from urothelial proliferation and differentiate into low-grade noninvasive papillary tumors. However, current genome-wide expression and sequencing studies have identified genes and pathways which are clear drivers in urothelial most cancers growth. A more advanced picture with molecular subclasses that are agnostic to standard tumor stage and grade has emerged. Proposed schema of expression-based, subtype-stratified therapeutic approach as a framework for prospective hypothesis testing in clinical trials. Ultimately, grouping bladder cancer into distinct molecular clusters may help identify certain sufferers that may profit from particular therapies. Similar to typical luminal tumors, a subset of micropapillary cancers reveal activation of wild-type p53, and these represent the most aggressive phenotypes with the worst prognosis (Guo et al. Recently, a wider spectrum of histologic variants of urothelial cancer has been recognized and investigated that includes distinct progress patterns of urothelial carcinoma, altered mobile differentiation of stromal reactions, and distinctive responses to therapy and external stimuli. Micropapillary Variant Micropapillary urothelial carcinoma was first described in 1994 and happens in roughly zero. There is a powerful male predominance related to micropapillary urothelial cancer, with stories of a male-to-female ratio as excessive as 37:1. Micropapillary urothelial carcinoma is related to advanced illness, as more than 50% are stage T3 or T4 at analysis; as such 5- and 10-year overall survival is 51% and 24%, decrease than with other widespread histologies (Kamat et al. However, even amongst lower-stage bladder tumors, micropapillary variant is associated with a worse prognosis because these tumors are associated with a progression fee from non�muscle-invasive to muscle-invasive disease of 70%, with a excessive subsequent metastatic price regardless of therapy (Kamat et al. Histologically, micropapillary urothelial carcinoma exhibit small tight clusters or thin papillae of atypical cells with eosinophilic to clear cytoplasm surrounded by distinguished retraction artifact (Watts and Hansel, 2010). Unlike other histologic subtypes, any quantity of micropapillary urothelial carcinoma could also be current for it to be defined as micropapillary and clinically managed as such. The best therapy for all stages of micropapillary urothelial carcinoma is surgical resection. Patients with the sarcomatoid variant are seen with massive infiltrative plenty, often at higher stages with a 5-year cancer-specific survival as little as 28. Plasmacytoid Variant the plasmacytoid variant of urothelial carcinoma is rare, comprising less than 1% of all urothelial tumors (Lopez-Beltran et al. The plasmacytotic variant microscopically has increased eosinophilic cytoplasm, with eccentrically positioned and enlarged hyperchromatic nuclei. These tumors usually are seen in a sophisticated stage with deep invasion into the bladder muscle and perivesical tissues, and with attribute intraperitoneal metastatic spread. Although plasmacytoid variant is chemosensitive and thus treated with neoadjuvant chemotherapy whenever potential, relapses are frequent with median survival amongst nonmetastatic sufferers simply 17. Although the nested variant is often upstaged at the time of cystectomy and located to be domestically advanced on the time of presentation, stage-matched comparisons between nested variant and pure urothelial carcinoma suggest comparable rates of recurrence and survival (Beltran et al. Urothelial Carcinoma With Divergent Differentiation Urothelial carcinoma with squamous differentiation is current in up to 16% to 22% of patients with bladder most cancers, though these could additionally be underestimates, and research counsel that up to 60% of bladder cancers have squamous elements (Black et al. The under-reporting of squamous differentiation and the p.c of the tumor involved make it difficult to assess how this divergent histology affects clinical outcomes (Shah et al. Squamous differentiation is related to the basal molecular subtype of bladder most cancers, which is seen at a extra advanced stage and is more focally aggressive (Choi et al. These tumors could additionally be associated with recurrence and progression for patients with localized and superior levels (Li et al. Glandular differentiation comprises small tubular or gland-like spaces in otherwise typical urothelial carcinoma and is current in approximately 10% of sufferers with urothelial bladder cancer.
Eight of them achieved complete daytime continence anxiety young living amitriptyline 50 mg cheap otc, similar to anxiety 9 months after baby discount 50 mg amitriptyline overnight delivery results anticipated in nonirradiated patients upsloping st depression exercise test cheap amitriptyline 25 mg visa. Early and late outcomes were much like these in the bigger group of nonirradiated sufferers. It is obvious that orthotopic lower urinary tract reconstruction could be safely carried out in carefully chosen sufferers with a historical past of prior full-dose pelvic irradiation. Even selected women with a historical past of pelvic irradiation could also be appropriate candidates for orthotopic reconstruction with good clinical outcomes (Lee et al. However, these are challenging procedures that clearly require technical experience and keen intraoperative judgment. Previous high-dose prostate radiation (external beam or brachytherapy) or a vaginal implant for cervical cancer trigger extra scarring within the rhabdosphincter area than does external-beam radiation for both bladder most cancers or other malignancies. Permanent brachytherapy seeds used for prostate cancer treatment usually find yourself within the levator muscles and urogenital diaphragm and will end in extreme scarring around the area of the exterior sphincter. Preoperative evaluation together with cystoscopy is helpful to consider the integrity of the mucosa around the space of the sphincter. However, it will not be possible to accurately predict the diploma of radiation damage discovered at surgical procedure, so careful intraoperative tissue assessment and determination of the situation of the urethra, ureters, and bowel should be carried out to make a ultimate decision concerning the feasibility of orthotopic diversion (Abbas et al. These patients should all the time be recommended preoperatively that the orthotopic diversion will not be potential. Acute upper tract obstruction brought on by the tumor usually ends in a transient rise in creatinine, which might be expected to improve after cystectomy and must be taken into consideration when counseling sufferers. In truth, an overweight patient may at occasions be higher served with orthotopic diversion because of the issue developing a functional conduit stoma with a really thick stomach wall. Manual Dexterity and Willingness to Do Self-Catheterization the want to do occasional or routine self-catheterization is reported in 10% to 20% of men and in as much as 30% to 60% of girls (see later). Thus all sufferers thought of for continent diversion ought to be prepared and able to do self-catheterization. This is especially necessary in women, in whom the potential need to do self-catheterization is larger and typically technically tougher than in men. Urethral Stricture Disease or External Sphincter Damage Severe urethral stricture disease in men and women is a contraindication for orthotopic diversion. Poor exterior sphincter perform in a person who is very motivated to bear orthotopic diversion could also be managed with a concomitant or delayed synthetic urinary sphincter system (Simma-Chiang et al. Similarly, a woman with vital stress incontinence might bear a concomitant Burch or pubourethral sling process, although she is more doubtless to be dependent on intermittent catheterization to drain correctly if this is accomplished. Patients with prior radiation are at elevated threat for several complications, even with an ileal conduit diversion. Kim and Steinberg (2001) discovered an elevated risk for surgical complications, particularly people who required percutaneous or surgical intervention, in 23 patients undergoing cystectomy and conduit after radiation compared with 23 matched controls. They discovered that ureteroileal issues occurred in 9% of sufferers by 5 years and concluded that it was not essential to use transverse colon for diversion in these patients. The problems and ultimate useful consequence of orthotopic neobladders in sufferers with prior pelvic radiation have been evaluated by numerous authors. Nine sufferers had truthful or poor continence earlier than surgery, and 6 of those underwent synthetic sphincter placement both on the time of cystectomy or afterward. However, eleven of the 13 males with good preoperative continence, including 1 who had each radical prostatectomy and radiation, regained good continence (0 or 1 pad Chapter 141 per day) after neobladder construction. One problem in these surgeries is to establish the prior vesicourethral anastomosis to make positive that the bladder is completely resected. Flexible cystoscopy at the time of the apical dissection can help on this regard. In conclusion, with cautious dissection a affected person who was continent after the preliminary radical prostatectomy surgical procedure can be anticipated to have a suitable outcome with a neobladder. A patient with multiple prior bowel resections may be at risk for growing continual diarrhea and even short bowel syndrome after a further 45 to 60 cm of small bowel is resected. In these patients, alternate options to orthotopic diversion similar to a sigmoid neobladder might be entertained. In common, prior bowel resections may be managed by rigorously dissecting out the entire small bowel, taking down any adhesions before performing the diversion. It is crucial to determine the old bowel anastomosis and, every time attainable, take it down and use that website as one end of the continent reservoir. This avoids potential devascularization of the bowel section between the old and new bowel anastomoses. Orthotopic Urinary Diversion 3239 direct contact with the fibers of the levator ani muscle. Rather, the male rhabdosphincter can be "omega-shaped" primarily ventral and lateral to the membranous urethra and prostate. The innervation of the male rhabdosphincter was additionally found to originate from fantastic branches that come up off the pudendal nerve. These authors advised that harm to both the rhabdosphincter or the pudendal innervation may impair the sphincter mechanism in males. Minimal manipulation of the tissue across the urethra-corresponding innervation is essential to offering optimum urinary continence (Colleselli et al. Most urologists are familiar with these strategies in male sufferers from their experience with radical prostatectomy. They may be much less familiar with the dissection of the urethra and bladder neck in girls. In a normal cystectomy, the bladder and prostate are completely freed off the rectum and mobilized posteriorly earlier than the urethral dissection. If a nerve-sparing method is planned, the urethra may be divided after the lateral pedicles are taken down to the bladder (anterior branches of the inner iliac vessels). The prostate is then dissected in a retrograde style off the rectum and bilateral neurovascular bundles, and the posterior pedicles are divided final. In both method, all fibroareolar connections alongside the anterior bladder wall, prostate, and undersurface of the pubic symphysis are divided. The endopelvic fascia is incised adjoining to the prostate, and the levator muscle tissue are gently swept off the lateral and apical portions of the prostate. The superficial department of the deep dorsal vein is recognized, ligated, and divided. The puboprostatic ligaments must be incised solely sufficient to allow proper apical dissection of the prostate. We use absorbable suture to keep away from the chance for erosion of suture, clips, or staples into the urethral anastomosis. Any bleeding from the transected venous complicated can be managed with an absorbable suture. Care ought to be taken to keep away from deep suture bites into the complex or levator muscles, which could injure the continence mechanism. Six 2-0 absorbable monofilament or woven polyglycolic acid sutures are placed in the urethra circumferentially under direct imaginative and prescient before full division of the urethra, rigorously incorporating solely the wall of the urethra with out including the levator muscles. Placing the urethral sutures presently rather than after the bladder has been removed avoids the retraction of the urethra that makes subsequent correct placement tough. Two additional sutures are then placed, incorporating the rectourethralis muscle posteriorly and the caudal extent of the Denonvilliers fascia. The urethral sutures are tagged to establish their location and are positioned underneath a towel till the urethroenteric anastomosis is carried out. The surgical dissection at the prostatic apex in men and bladder neck in ladies should be rigorously and exactly performed to obtain optimum continence whereas taking care to not compromise the oncologic effectiveness of the surgery. In both males and females, the urethral sphincter is made up of both easy and striated muscle tissue. The striated rhabdosphincter appears to be the most important for continence and is innervated by the pudendal nerve. Careful neuroanatomic dissections with three-dimensional reconstructions of female and male cadavers have defined the anatomy of the urethral sphincter mechanism (Borirakchanyavat et al. No clearly defined line could be identified between the transverse easy muscle cranially and the striated muscle caudally. Rather, a gradual transition was noted in the center third of the urethra, with intermingling fibers of each kinds of muscle.
The prognosis for patients with these tumors has been traditionally reported as poor (Das and Amar mood disorder clinic cleveland ohio 50 mg amitriptyline buy visa, 1986; Faysal and Freiha depression hallucinations cheap amitriptyline 50 mg online, 1981; Melekos et al depression symptoms speech cheap amitriptyline 25 mg overnight delivery. The poor prognosis has been attributed to delayed prognosis and superior stage at presentation (Faysal and Freiha, 1981; Fellows, 1978; Mii and Ili, 1983; Ostroff et al. Historically, this has supported the prophylactic surgical remedy of all bladder diverticula, including asymptomatic and minimally symptomatic lesions (Kelalis and McLean, 1967). It has been instructed that medical stage at presentation is the most important prognostic issue for sufferers with tumors in bladder diverticula, with 5-year actuarial survival ranging from 83% � 9% in patients with superficial disease to 45% � 14% in those with extradiverticular illness (Golijanin et al. One small collection means that aggressive individualized multimodal therapy in these patients, including surgical procedure, chemotherapy, and radiation remedy, might enhance prognosis (Garzotto et al. Because pathological staging after transurethral resection is difficult and often inaccurate, some authors have instructed a really aggressive strategy to these tumors. This surgical staging method includes an open exploration and partial or radical cystectomy with no prior transurethral resection (Redman et al. Others have advocated a selective individualized approach, taking Bladder and Female Urethral Diverticula 2971 under consideration the scientific stage and pathological grade of the tumor (Golijanin et al. Radical cystectomy has similar outcomes for tumors inside diverticula as for tumors in other areas. Low-grade, low-stage tumors could additionally be efficiently treated with diverticulectomy alone (Baniel and Vishna, 1997; Bourgi et al. As famous earlier, the potential threat of perforation with transurethral resection is greater with these tumors due to the lack of an outlined muscularis propria layer. However, whether these sufferers can be safely treated with biopsy and fulguration with or without intravesical chemotherapy/ immunotherapy and interval cystoscopic surveillance for low-grade tumors, is unclear. Other Associated Conditions the placement of many bladder diverticula on the level of the ureterovesical junction might explain the excessive incidence of associated ipsilateral ureteral abnormalities. A very high prevalence of ipsilateral vesicoureteral reflux has been noted in association with congenital bladder diverticula (Amar, 1972; Barrett et al. Other concerns in the analysis and management of bladder diverticula embody the potential improvement of stones within the diverticulum, ureteral obstruction (Bellinger et al. However, simultaneous open bladder diverticulectomy/open prostatectomy in addition to simultaneous bladder diverticulectomy/transurethral prostatectomy may be carried out (Porpiglia et al. Transurethral resection of the diverticular neck has been reported to achieve success in select circumstances (Vitale and Woodside, 1979). The neck of the diverticulum is incised utilizing the resectoscope loop or Collins knife. Incisions are carried right down to the muscular fibers of the bladder at the degree of the ostium of the diverticulum. When successful, this procedure enlarges the neck of the diverticulum, disrupting the slender sphincteric-like properties of its connection to the bladder lumen and thereby permitting improved emptying of the diverticulum during micturition. Although typically secure and nicely tolerated, this technique has resulted in urinary retention because of a reversal of circulate throughout micturition and "venting" of the bladder contents into the diverticulum postoperatively (Schulze and Hald, 1983). This method has been reported to be less successful in those individuals with massive diverticula (Orandi, 1977; Vitale and Woodside, 1979). Transurethral resection of the diverticular neck could also be combined with fulguration of the entire urothelial lining of the diverticulum (Adachi et al. Fulguration of the liner of the diverticulum should end in obliteration of the diverticulum or a considerable discount in its size. Observation and Nonsurgical Management Adult patients with minimal signs and no complicating elements may go for statement with surveillance. These sufferers ought to be endorsed regarding the potentially increased danger of malignancy and the necessity for periodic reassessment in addition to the unpredictable course and probably aggressive nature of malignancy if subsequently found in this setting. Indications for bladder diverticulectomy in kids are much like these in adults. However, in kids with a number of bladder diverticula related to a chromosomal syndrome, observation and medical management are often most popular because of the inherent connective tissue disorders found in these sufferers, which impair postoperative wound therapeutic, improve perioperative surgical danger, and predispose to recurrence (Psutka and Cendron, 2013). Operative Excision Operative excision could also be performed through an open, laparoscopic, or robotic approach with or without concomitant therapy of associated bladder outlet obstruction. Indications for Intervention Many sufferers with by the way found congenital or acquired bladder diverticula are managed expectantly and with periodic surveillance. Bladder diverticula can range tremendously in size and, in some situations, are bigger than the bladder. Symptoms or complications related to bladder diverticula are most often as a outcome of poor emptying of the diverticulum and urinary stasis. Therefore excision of the diverticula can be expected to improve emptying of the decrease urinary tract, supplied that the primary downside that resulted in the formation of the bladder diverticulum. The relative merits of surgical excision versus surveillance must be fastidiously thought of and discussed with every patient individually. Such lesions characterize a few of the most difficult diagnostic and reconstructive issues in female urology. Ureth ral lu men related to incontinence, stones, extreme dyspareunia, and/or tumors. Anatomic variations between patients and within the location, size, and complexity of those lesions make positive that each case is unique. A printed series of 121 cases by Davis and TeLinde (1958) approximately doubled the variety of instances reported in the course of the previous 60 years. Periurethral glands are situated inside the submucosa of the urethra deep to the muscular envelope, draining distally however arborizing proximally. Anatomy of the Female Urethra the traditional feminine urethra is a musculofascial tube roughly three to four cm in length, extending from the bladder neck to the exterior urethral meatus, suspended from the pelvic sidewall and pelvic fascia (tendinous arc of the obturator muscle) by a sheet of connective tissue known as the urethropelvic ligament. This structure may be considered to have an stomach side (the endopelvic fascia) and a vaginal side (the periurethral fascia). The urethral lumen is lined by a urothelial layer proximally and a nonkeratinized stratified squamous cell type distally. The urethra could additionally be conceptualized as a wealthy, vascular, spongy cylinder surrounded by an envelope consisting of smooth and skeletal muscle and fibroelastic tissue (Young and Wahle, 1996). The Skene glands are the largest and most distal of those glands and are generally known as the paraurethral glands. These paraurethral glands drain outside the urethral lumen, lateral to the urethral meatus. The urethra has several muscular layers: an inner longitudinal clean muscle layer, an outer round clean muscle layer, and a skeletal muscle layer. The skeletal muscle component spans a lot of the size of the urethra but is extra outstanding within the center third. The proximal urethra has a blood provide much like the adjoining bladder, whereas the distal urethra derives its blood supply from the terminal branches of the inferior vesical artery through the vaginal artery that runs along the superior lateral side of the vagina (Hinman, 1993). Lymphatic drainage of the feminine urethra is to the external and internal iliac nodes from the proximal urethra and to the superficial and deep inguinal lymph nodes from the distal urethra. Innervation to the female urethra is from the pudendal nerve (S2 to S4), and afferents from the urethra travel by way of the pelvic splanchnic nerves. These glands are normally found within the submucosal layer of the spongy tissue of the distal two-thirds of the urethra. Repeated infection and abscess formation in these obstructed glands finally lead to enlargement and growth. Initially the expanding mass displaces the spongy tissue of the urethral wall and then enlarges to disrupt the muscular envelope of the urethra. The enlarging cavity can then increase and dissect within the leaves of the periurethral fascia and urethropelvic ligament. Diverticula in the pediatric population have been attributed to a selection of congenital anomalies, including an ectopic ureter draining right into a Gartner duct cyst and a forme fruste of urethral duplication (Boyd and Raz, 1993; Silk and Lebowitz, 1969; Vanhoutte, 1970). By reviewing 10-�m transverse sections, he refuted earlier anatomic descriptions of the glandular anatomy of the female. Furthermore, he noted that periductal and interductal irritation was found generally. However, the initial infection and, especially, subsequent reinfections may originate from quite a lot of sources, including Escherichia coli and other coliform bacteria as nicely as vaginal flora. Reinfection, inflammation, and recurrent obstruction of the neck of the cavity are theorized to lead to patient signs and enlargement of the diverticulum. A population-based study of women in Olmstead County, Minnesota, by El-Nashar et al.
It is a silicone system containing a miniature inside pump out there in lengths starting from three to 7 cm and diameter of 24 or 28 Fr depression la definition amitriptyline 50 mg buy discount line. Initial sizing and placement is performed by the physician and have to be changed each 29 days depression symptoms after quitting smoking 25 mg amitriptyline discount otc. The device is inserted into the urethra using a disposable introducer and fixed in place by silicone fins at the level of the bladder neck and a versatile flange at the urethral meatus anxiety xanax not working amitriptyline 25 mg generic mastercard. To void, the affected person locations a distant control (inFlow activator) over the suprapubic space and presses a button, which magnetically activates an inside pump to generate a urine move of 10 to 12 mL/s. With a protocol of pre-insertion patient training and post-insertion nursing help, a better price of gadget acceptance may be achieved (Lynch et al. Stimulated Myoplasty for Bladder Emptying Few treatment options can be found for patients with detrusor underactivity apart from self-intermittent catheterization. Restoration of bladder contractility stays an elusive objective for many patients with this situation. The first animal feasibility research to augment bladder contractility used a unilateral rectus abdominis muscle wrap over the bladder to facilitate bladder emptying (Chancellor et al. The rectus muscle, with intact neurovascular pedicle, was dissected free at one finish and wrapped over the bladder to create a spherical configuration housing the bladder. Evaluation of the transposed muscle showed no injury to the blood provide or innervation of the rectus muscle, and the underlying bladder retained its quantity despite neurogenically induced underactivity. This mannequin was touted because the precursor for a medical trial by which the patient would study to contract his rectus muscle voluntarily and create enough extrinsic stress to void. One month later, the patient could void by contracting his rectus muscle, producing 50 cm H2O detrusor strain. This ability continued for 11 months till the case was reported within the literature. At 6 months, the authors demonstrated a statistically significant decrease in postvoid residual and statistically significant will increase in urine circulate rate, bladder contractility, and detrusor strain. The benefit of a singular nerve supply with ample geometry offered by the latissimus dorsi free flap led to the primary medical software in 1998 by Stenzl et al. Three patients with bladder acontractility have been handled with latissimus dorsi myoplasty, and all three had been capable of void by belly straining. In a larger scientific research utilizing the free switch of the latissimus dorsi muscle to restore voluntary voiding, 14 of 20 sufferers were in a position to void spontaneously with postvoid residual volumes of less than one hundred mL (Ninkovic et al. The largest latissimus dorsi detrusor myoplasty expertise was reported by Gakis et al. Three patients decreased the frequency of catheterization by 50%, and four patients had no enchancment. However, in some instances, sufferers have failed multiple anti-incontinence procedures and exterior amassing devices or pads are the only administration options out there. External Collecting Devices No exterior urinary collecting system for females has been successful or effective. However, external accumulating gadgets for men-the condom catheter, penile sheath, or Texas catheter-are usually effective in urine assortment. Patients additionally reported that external urinary collection devices have been extra snug and fewer restrictive on day by day activities than indwelling catheters. Furthermore, the penile pores and skin and glans must be examined at each catheter change to guarantee no pores and skin breakdown or contact reactions have occurred (Newman, 1999). These devices have the potential to trigger strain necrosis of the penis and, when severe, could even harm the urethra (Golji, 1981). External urine collecting units also are susceptible to dislodge or fall off, especially if the affected person is carrying an inappropriate measurement. Absorbent Products Urinary incontinence could be a socially debilitating downside resulting in worry of odor, discovery, and embarrassment. Many sufferers with urinary incontinence put on some kind of absorbent product, which may include pads, shields, drip collectors, guards, undergarments, briefs, diapers, or underpads. More research is required to evaluate the impact of these parameters on value and quality of care. Often recognized because the authority in the management of the incontinent patient, urologists ought to acknowledge the basic nursing principles and skin care suggestions that will considerably contribute to patient care. Absorbent products should be modified frequently to help avoid buildup of odor and limit publicity of the skin to urine. Treatment strategies are quite a few and sometimes mix medical and surgical administration. Baker J, Norton P: Evaluation of absorbent merchandise for girls with gentle to average urinary incontinence, Appl Nurs Res 9:29�33, 1996. Bugel H, Pfister C, et al: Intraurethral macroplastic injections within the treatment of urinary incontinence after prostatic surgical procedure, Prog Urol 9(6):1068�1076, 1999. Colombo T, Augustin H, Breinl E, et al: the usage of polydimethylsiloxane in the treatment of incontinence after radical prostatectomy, Br J Urol 80(6):923�926, 1997. Corcos J, Fournier C: Periurethral collagen injection for the therapy of female stress urinary incontinence: 4-year follow-up outcomes, Urology 54(5):815�818, 1999. Delnay K, Stonehill W, Goldman H, et al: Bladder histological modifications related to continual indwelling urinary catheter, J Urol 161:1106�1109, 1999. Edlund C, Peeker R, Fall M: Clam ileocystoplasty: successful remedy of severe bladder overactivity, Scand J Urol Nephrol 35:190�195, 2001. Freton L, Tondut L, Enderle I, et al: Comparison of adjustable continence remedy periurethral balloons and synthetic urinary sphincter in feminine sufferers with stress urinary incontinence as a end result of intrinsic sphincter deficiency, Int Urogynecol J 2018. Gakis G, Ninkovic M, Gommert A, et al: Functional detrusor myoplasty for bladder acontractility: long-term outcomes, J Urol 185:593�599, 2011. Gerullis H, Eimer C, Georgas E, et al: Muscle-derived cells for treatment of iatrogenic sphincter harm and urinary incontinence in males, ScientificWorldJournal 2012:898535, 2012. Getliffe K, Fader M, Cottenden A, et al: Absorbent merchandise for incontinence: "remedy results" and impact on quality of life, J Clin Nurs sixteen:1936�1945, 2007. Ghoniem G, Corcos J, Comiter J, et al: Cross-linked polydimethylsiloxane injection for feminine stress urinary incontinence: outcomes of a multicenter, randomized, controlled, single-blind research, J Urol 181(1):204�210, 2009. Ghoniem G, Corcos J, Comiter C, et al: Durability of urethral bulking agent injection for female stress urinary incontinence: 2-year multicenter research results, J Urol 183(4):1444�1449, 2010. Kavanagh A, Afshar K, Scott H, et al: Bladder neck closure in conjunction with enterocystoplasty and Mitrofanoff diversion for complex incontinence: closing the door for good, J Urol 188:1561�1565, 2012. Khastgir J, Hamid R, Arya M, et al: Surgical and affected person reported outcomes of "clam" augmentation ileocystoplasty in spinal cord injured patients, Eur Urol forty three:263�269, 2003. Kocjancic E, Crivellaro S, Ranzoni S, et al: Adjustable Continence Therapy for severe intrinsic sphincter deficiency and recurrent feminine stress urinary incontinence: long-term expertise, J Urol 184(3):1017�1021, 2010. Kuismanen K, Sartoneva R, Haimi S, et al: Autologous adipose stem cells in therapy of female stress urinary incontinence: results of a pilot research, Stem Cells Transl Med 3(8):936�941, 2014. Kylmala T, Tainio H, Raitanen M, et al: Treatment of postoperative male urinary incontinence using transurethral Macroplastique injections, J Endourol 17(2):113�115, 2003. Lapides J, Diokno A, Silber S, et al: Clean intermittent self-catheterization in the therapy of urinary tract disease, J Urol 107:458�465, 1972. Lightner D, Calvosa C, Andersen R, et al: A new injectable bulking agent for therapy of stress urinary incontinence: outcomes of a multicenter, randomized, controlled, double-blind research of Durasphere, Urology 58(1):12�15, 2001. Lightner D, Rovner E, Corcos J, et al: Randomized managed multisite trial of injected bulking agents for ladies with intrinsic sphincter deficiency: mid-urethral injection of Zuidex via the Implacer versus proximal urethral injection of Contigen cystoscopically, Urology 74(4):771�775, 2009. Gotoh M, Yamamoto T, Kato M, et al: Regenerative therapy of male stress urinary incontinence by periurethral injection of autologous adipose-derived regenerative cells: 1-year outcomes in eleven sufferers, Int J Urol 21(3):294�300, 2014. Gras S, Klarskov N, Lose G: Intraurethral injection of autologous minced skeletal muscle: a easy surgical therapy for stress urinary incontinence, J Urol 192(3):850�855, 2014. Guttmann L, Frankel H: the worth of intermittent catheterisation within the early administration of traumatic paraplegia and tetraplegia, Paraplegia 4:63�83, 1966. Halachmi S, Farhat W, et al: Efficacy of polydimethylsiloxane injection to the bladder neck and leaking diverting stoma for urinary continence, J Urol 171(3):1287�1290, 2004. Hamid R, Bycroft J, Arya M, et al: Screening cystoscopy and biopsy in sufferers with neuropathic bladder and chronic suprapubic indwelling catheters: is it legitimate Hurtado E, McCrery R, Appell R: the security and efficacy of ethylene vinyl alcohol copolymer as an intra-urethral bulking agent in girls with intrinsic urethral deficiency, Int Urogynecol J Pelvic Floor Dysfunct 18(8):869�873, 2007.
Liapis A depression symptoms with anxiety order 50 mg amitriptyline overnight delivery, Bakas P depression symptoms withdrawal 25 mg amitriptyline buy with visa, Christopoulos P prenatal depression symptoms quiz 25 mg amitriptyline generic with visa, et al: Tension-free vaginal tape for aged girls with stress urinary incontinence, Int J Gynaecol Obstet 92:48�51, 2006. Liapis A, Bakas P, Creatsas G: Burch colposuspension and tension-free vaginal tape within the administration of stress urinary incontinence in girls, Eur Urol forty one:469�473, 2002. Lieb J, Das A: Urethral erosion of tension-free vaginal tape, Scand J Urol Nephrol 37:184�185, 2003. Lo T, Horng S, Chang C, et al: Tension-free vaginal tape procedure after earlier failure in incontinence surgical procedure, Urology 60:57�61, 2002. Madjar S, Tchetgen M, Van Antwerp A, et al: Urethral erosion of tension-free vaginal tape, Urology 59:601, 2002. One 12 months information from a multi-centre prospective trial, Int Urogynecol J 20:313�317, 2009. Meschia M, Pifarotti P, Bernasconi F, et al: Tension-free vaginal tape: evaluation of outcomes and problems in 404 stress incontinent girls, Int Urogynecol J Pelvic Floor Dysfunct 12(Suppl 2):S24�S27, 2001. Meschia M, Rossi G, Bertini S, et al: Single incision mid-urethral slings: impact of weight problems on outcomes, Eur J Obstet Gynecol Reprod Biol 170:571�574, 2013. Minaglia S, Ozel B, Hurtado E, et al: Effect of transobturator tape process on proximal urethral mobility, Urology sixty five:55�59, 2005. Minaglia S, Ozel B, Klutke C, et al: Bladder injury throughout transobturator sling, Urology 64:376�377, 2004. Minaglia S, Urwitz-Lane R, Wong M, et al: Effectiveness of transobturator tape in women with decreased urethral mobility, J Reprod Med 54:15�19, 2009. Mitsui T, Tanaka H, Moriya K, et al: Clinical and urodynamic outcomes of pubovaginal sling process with autologous rectus fascia for stress urinary incontinence, Int J Urol 14:1076�1079, 2007. Mostafa A, Agur W, Abdel-All M, et al: Multicenter potential randomized examine of single-incision mini-sling vs. Mustafa M, Wadie B: Bladder erosion of tension-free vaginal tape introduced as vesical stone; administration and review of literature, Int Urol Nephrol 39:453�455, 2007. A randomized trial of urodynamic testing before stress-incontinence surgery, N Engl J Med 366:1987�1997, 2012. Negoro H, Kawakita M, Imai Y: Intravesical tape erosion following the tensionfree vaginal tape procedure for stress urinary incontinence, Int J Urol 12:696�698, 2005. Novara G, Galfano A, Boscolo-Berto R, et al: Complication charges of tension-free midurethral slings in the treatment of feminine stress urinary incontinence: a systematic evaluate and meta-analysis of randomized controlled trials comparing tension-free midurethral tapes to different surgical procedures and completely different devices, Eur Urol 53:288�308, 2008. Oh T, Ryu D: Transurethral resection of intravesical mesh after midurethral sling procedures, J Endourol 23:1�5, 2009. Onur R, Singla A: Solvent-dehydrated cadaveric dermis: a new allograft for pubovaginal sling surgery, Int J Urol 12:801�805, 2005. Ozel B, Minaglia S, Hurtado E, et al: Treatment of voiding dysfunction after transobturator tape procedure, Urology 64:1030, 2004. Sanders R, Genadry R, Yang A, et al: Imaging the female urethra with ultrasound, Ultrasound Q 12:167�183, 1994. Paraiso M, Walters M, Karram M, et al: Laparoscopic Burch colposuspension versus tension-free vaginal tape: a randomized trial, Obstet Gynecol 104:1249�1258, 2004. Bilateral bladder erosion of a transobturator tape mesh, Obstet Gynecol 108:713�715, 2006. Partoll L: Efficacy of tension-free vaginal tape with different pelvic reconstructive surgical procedure, Am J Obstet Gynecol 186:1292�1298, 2002. Experience from the British Society of Urogynaecology database and literature review, J Obstet Gynaecol 31:514�517, 2011. Persson J, Teleman P, Eten-Bergqvist C, et al: Cost-analyses based mostly on a prospective, randomized study comparing laparoscopic colposuspension with tension-free vaginal tape procedure, Acta Obstet Gynecol Scand 81:1066�1073, 2002. Petros P, Ulmsten U: An integral principle of female urinary incontinence: experimental and medical concerns, Acta Obstet Gynecol Scand 69(S153):7�31, 1990. Pit M: Rare complications of tension-free vaginal tape process: late intraurethral displacement and early misplacement of tape, J Urol 167:647, 2002. Porena M, Constantini E, Frea B, et al: Tension-free vaginal tape versus transobturator tape as surgery for stress urinary incontinence: outcomes of a multicentre randomised trial, Eur Urol fifty two:1481�1491, 2007. Powers K, Lazarou G, Greston W: Delayed urethral erosion after tension-free vaginal tape, Int Urogynecol J 17:422�425, 2006. Rautenberg O, Kociszewski J, Welter J, et al: Ultrasound and early tape mobilization-a sensible answer for treating postoperative voiding dysfunction, Neurourol Urodyn 33:1147�1151, 2014. Rechberger T, Rzeniczuk K, Skorupski P, et al: A randomized comparison between monofilament and multifilament tapes for stress incontinence surgery, Int Urogynecol J Pelvic Floor Dysfunct 14:432�436, 2003. Rehman J, Chugtai B, Sukkarieh T, et al: Extraperitoneal laparoscopic elimination of eroded midurethral sling: a new technique, J Endourol 22:365�368, 2008. Revicky V, Mukhopadhyay S, de Boer F, et al: Obesity and the incidence of bladder damage and urinary retention following tension-free vaginal tape procedure: retrospective cohort research, Obstet Gynecol Int 2011:746393, 2011. Chapter one hundred twenty five Segal J, Vassallo B, Kleeman S, et al: Prevalence of persistent de novo overactive bladder symptoms after the tension-free vaginal tape, Obstet Gynecol 104:1263�1269, 2004. Serati M, Ghezzi F, Cattoni E, et al: Tension-free vaginal tape for the treratment of urodynamic stress incontinence: efficacy and opposed results at 10-year follow-up, Eur Urol 61:939�946, 2012. Serati M, Braga A, Athanasiou S, et al: Tension-free vaginal tape-obturator for therapy of pure urodynamic stress urinary incontinence: efficacy and antagonistic results at 10-year follow-up, Eur Urol seventy one:674�679, 2017a. Sevestre S, Ciofu C, Deval B, et al: Results of the tension-free vaginal tape technique within the elderly, Eur Urol 44:128�131, 2003. Shah K, Nikolavsky D, Gilsdorf D, et al: Surgical administration of lower urinary mesh perforation after mid-urethral polypropylene mesh sling: mesh excision, urinary tract reconstruction and concomitant pubovaginal sling with autologous rectus fascia, Int Urogynecol J 24:2111�2117, 2013. Singla N, Aggarwal H, Foster J, et al: Management of urinary incontinence following suburethral sling elimination, J Urol 198:644�649, 2017. Slack M, Sandhu J, Staskin D, et al: In vivo comparability of suburethral sling supplies, Int Urogynecol J Pelvic Floor Dysfunct 17:106�110, 2005. Song P, Wen Y, Huang C, et al: the efficacy and security comparison of surgical therapies for stress urinary incontinence: a community meta-analysis, Neurourol Urodyn 37:1199�1211, 2018. Staskin D, Bavendam T, Miller J, et al: Effectiveness of a urinary management insert within the management of stress urinary incontinence: early outcomes of a multicenter study, Urology forty seven:829�836, 1998. Stoeckel W: Uber die Verwendung der Musculi pyramidales bei der operativen Behandlung der Incontinentia Urinae, Zentralbl Gynakol 41:11�19, 1917. Subak L, Wing R, West D, et al: Weight loss to deal with urinary incontinence in overweight and obese women, N Engl J Med 360:481�490, 2009. Sweat S, Itano N, Clemens J, et al: Polypropylene mesh tape for stress urinary incontinence: problems of urethral erosion and outlet obstruction, J Urol 168:144�146, 2002. Tahseen S, Reid P: Effect of transobturator tape on overactive bladders signs and urge urinary incontinence in ladies with blended urinary incontinence, Obstet Gynecol 113:617�623, 2009. Tamussino K, Hanzal E, K�lle D, et al: Tension-free vaginal tape operation: outcomes of the Austrian registry, Obstet Gynecol 98:732�736, 2001. Tamussino K, Hanzal E, K�lle D, et al: Transobturator tapes for stress urinary incontinence: outcomes of the Austrian registry, Am J Obstet Gynecol 197:634. Teo R, Moran P, Mayne C, et al: Randomized trial of tension-free vaginal tape and tension-free vaginal tape-obturator for urodynamic stress incontinence in women, J Urol 185:1350�1355, 2011. Thompson R: A case of epispadias associated with full incontinence handled by rectus transplantation, Br J Dis Child 20:146�151, 1923. Tran H, Rutman M: Female outlet obstruction after anti-incontinence surgical procedure, Urology 112:1�5, 2018. Weltz V, Guldberg R, Lose G: Efficacy and perioperative security of synthetic mid-urethral slings in overweight girls with stress urinary incontinence, Int Urogynecol J 26:641�648, 2015. Westby M, Asmussen M, Ulmsten U: Location of most intraurethral pressure related to urogenital diaphragm in the female studied by simultaneous urethrocystometry and voiding urethrocystography, Am J Obstet Gynecol 144:408�412, 1982. Wiedemann A, Otto M: Small intestinal submucosa for pubourethral sling suspension for the remedy of stress incontinence: first histopathological leads to humans, J Urol 172:215�218, 2004. Wlazlak E, Viereck V, Kociczewski J, et al: Role of intrinsic sphincter deficiency with and without urethral hypomobility on the result of tape insertion, Neurourol Urodyn 36:1910�1916, 2017. Wolter C, Starkman J, Scarpero H, et al: Removal of transobturator midurethral sling for refractory thigh pain, Urology seventy two:461. Wyczolkowski M, Klima W, Piasecki Z: Reoperation after difficult tensionfree vaginal tape procedures, J Urol 166:1004�1005, 2001. Yenilmez A, Baseskioglu B, Kaya C: Groin abscess because of a forgotten midurethral sling connector, Int Urogynecol J 24:1059�1061, 2013.
However depression anger test generic amitriptyline 25 mg fast delivery, a minority of sufferers might best be managed by formal gastrostomy decompression inserted intraoperatively depression pathophysiology buy amitriptyline 50 mg without a prescription. These individuals embody these with multiple prior belly procedures in whom extended ileus is more probably depression cherry order 50 mg amitriptyline otc. If the affected person is nutritionally depleted preoperatively, hyperalimentation has been instructed to be of value if initiated in the course of the preoperative interval (Askanazi et al. A randomized controlled trial demonstrated that in nutritionally noncompromised sufferers, postoperative whole parenteral vitamin was related to increased infectious problems (Roth et al. Before manipulation, a urine sample from each stent should be sent for tradition and sensitivity testing. Before stent elimination, radiographs of the pouch could additionally be obtained to ensure that the pouch is unbroken. Retrograde ureteral studies may be carried out to guarantee towards ureteral anastomotic leakage. Each stent is injected with contrast agent in a seek for extravasation; if none is seen, information wires are advanced to every kidney, and the stents are removed. However, using ureteral retrograde research before stent elimination is by no means common, and several retrospective research have proven it to be of restricted worth (Pantuck et al. As a end result, urinary cytology should be performed for all sufferers present process a continent urinary diversion, whether or not the diversion was performed secondary to a urothelial malignancy. When the ureters are directed into the fecal stream, routine colonoscopy should also be carried out. Latency periods as brief as 5 years have been reported; due to this fact all patients growing gross or microscopic hematuria ought to be totally evaluated (Austen and Kalble, 2004; Golomb et al. If an anastomotic transitional cell most cancers is discovered, the patient should be absolutely evaluated with upper tract imaging and ureteroscopy if potential. For an isolated anastomotic recurrence, distal ureterectomy and reimplantation could also be acceptable. If nephroureterectomy is critical, some patients may require removal of their continent diversion because of resulting renal insufficiency. Analysis of the two affected person groups, then again, confirmed that these chosen for continent diversion were significantly youthful and 4 instances much less prone to have significant concurrent illness. What this evaluation suggests is that, with proper affected person choice, continent diversion operations may be safely performed with results just like those for conduit diversion. To decide if continent diversion might be safely performed in selected aged patients, Navon et al. The complication rates between the 2 groups had been acceptably low and surprisingly similar. Cutaneous Continent Urinary Diversion 3209 Rectal Bladder Urinary Diversion Various revolutionary surgical methods have been advocated for separating the fecal and urinary streams whereas still employing the rules of ureterosigmoidostomy. In basic, these operations can be mentioned together as rectal bladder urinary diversions. The proximal sigmoid colon is managed by terminal sigmoid colostomy or, extra commonly, by bringing the sigmoid to the perineum, thereby using the anal sphincter to obtain bowel and urinary management. The principal purpose is the potential for the calamitous complication of mixed urinary and fecal incontinence, presumably occurring as a consequence of harm to the anal sphincter mechanism through the dissection processes (Culp, 1984). If the urologist selects certainly one of these procedures, the preoperative analysis should embrace all the caveats of ureterosigmoidostomy. Anal sphincteric tone have to be judged competent before these operations are chosen. Our preference has been to use a 400- to 500-mL skinny mixture of oatmeal and water that the patient is requested to retain for 1 hour in the upright position (Spirnak and Caldamone, 1986). Finally, colonoscopy must be carried out earlier than the process to rule out preexisting colorectal disease, and surveillance should be ensured to monitor for subsequent development of colon cancer. Those looking for detailed descriptions of those procedures can find them in prior editions of this chapter. The following is a brief description of more fashionable surgical procedures that use the intact anal sphincter for urinary and fecal continence. However, the surgical strategies for these procedures are likewise not discussed in this version. Routine nightly insertion of a rectal tube is advocated within the long-term care of the patient. However, many patients will reject this follow as uncomfortable and unappealing. Functional results have been assessable in fifty seven sufferers: 1 died of a postoperative pulmonary embolism, and 6 died from their illness. All patients have been continent during the day with 2 to four emptyings, and all however four remained dry at evening with zero to 2 emptyings. Four youngsters skilled enuresis that responded to 25 mg of imipramine at bedtime. Two had been remedied by antegrade dilation, one was repaired by open revision, and one nonfunctioning renal unit was removed. Obviously, all sufferers undergoing these procedures have exposure of the urinary tract to fecal flora. Some authors advocate continual administration of an antibacterial agent to all such sufferers (Duckett and Gazak, 1983; Spirnak and Caldamone, 1986). Ureteral strictures require reoperative surgery and are skilled in 26% to 35% of patients over time (Duckett and Gazak, 1983; Williams et al. Barium enemas are relatively contraindicated as a outcome of reflux of this material into the kidneys (if the antireflux process fails) can be deleterious (Williams, 1984). Additional strategies for colon carcinoma screening on this inhabitants are the analysis of stool for blood and the tried cytologic examination of the blended urine and feces specimen (Filmer and Spencer, 1990). This operation is much like commonplace ureterosigmoidostomy except that a proximal intussusception of the sigmoid colon confines the urine to a smaller floor area, thus minimizing the issues of electrolyte imbalance. In addition, the rectum is patched with ileum to improve the urodynamic properties of the rectum as a urinary reservoir. The giant bowel ought to be studied for preexisting illness, and anal sphincteric integrity have to be tested earlier than surgical procedure. Folded Rectosigmoid Bladder A modification of the ureterointestinal anastomosis was described by a bunch from Mansoura, Egypt (El-Mekresh et al. This procedure creates a folded rectosigmoid bladder with anastomosis of the ureters by way of serosa-lined tunnels rather than into the taenia coli. This process has the advantage of a bigger sigmoid reservoir, as well as the prevention of reflux by creating the aforementioned serous-lined tunnel for the anastomosis. This reimplantation technique was first described by Abol-Enein and Ghoneim (1993) and appears to have a decrease complication rate than direct taenial implantation (Hafez et al. Patients undergoing this process should be intently monitored for the development of hyperchloremic acidosis. Because hypokalemia is also a characteristic of ureterosigmoidostomy, substitute of potassium along with bicarbonate may be achieved Hemi-Kock and T Pouch Procedures with Valved Rectum In his description of the augmented valved rectum procedure, Kock et al. After in depth experience with the Kock ileal reservoir, the group on the University of Southern California has tried to enhance on the intussuscepted Kock continence mechanism. The end result has been the modification of the T pouch to serve as an ileal anal reservoir (Stein et al. The wall of the ileum is closed over the T mechanism with a running absorbable suture. Postoperative management and problems associated with this operation are very related to these that could be experienced after any process that directs the urinary stream into the rectum. Radiologic research of the stents can be carried out after the seventh postoperative day. Before stent research are conducted, a Gastrografin enema may be performed by way of the rectal tube to be sure that the area of ureterocolonic anastomosis is unbroken, with follow-up movies to ensure immediate drainage of the upper urinary tracts into the rectosigmoid area. The patient is instructed to empty the colon at intervals of no extra than every 2 hours, significantly in the early postoperative period. When the rectal tube is removed, as in other situations when the urinary tract is diverted to the rectum, the patient should be carefully monitored for the development of hyperchloremic acidosis.
Booth J bipolar depression symptoms test free discount amitriptyline 50 mg overnight delivery, Hagen S molal depression constant definition 50 mg amitriptyline quality, McClurg D mood disorder medicine 25 mg amitriptyline with mastercard, et al: A feasibility study of transcutaneous posterior tibial nerve stimulation for bladder and bowel dysfunction in aged adults in residential care, J Am Med Dir Assoc 14:270�274, 2013. Bradway C, Miller E, Heivly A, et al: Continence care for obese nursing home residents, Urol Nurs 30:121�129, 2010. Brittain K, Perry S, Shaw C, et al: Isolated urinary, fecal, and double incontinence: prevalence and diploma of soiling in stroke survivors, J Am Geriatr Soc 54:1915�1919, 2006. Bylow K, Dale W, Mustian K, et al: Falls and bodily efficiency deficits in older patients with prostate most cancers undergoing androgen deprivation remedy, Urology seventy two:422�427, 2008. Bynum J, Song Y, Fisher E: Variation in prostate-specific antigen screening in males aged eighty and older in fee-for-service Medicare, J Am Geriatr Soc fifty eight:674�680, 2010. Daneman N, Gruneir A, Newman A, et al: Antibiotic use in long-term care facilities, J Antimicrob Chemother 66:2856�2863, 2011. Report from the 4th International Consultation on Incontinence, Neurourol Urodyn 29(1):165�178, 2010. Prospective ultrastructural/urodynamic analysis of its natural evolution, J Urol 157:1814�1822, 1997. Endeshaw Y: Correlates of self-reported nocturia amongst community-dwelling older adults, J Gerontol A Biol Sci Med Sci 64:142�148, 2009. Eriksson I, Gustafson Y, Fagerstrom L, et al: Urinary tract infection in very old women is related to delirium, Int Psychogeriatr 23:496�502, 2011. Ersoz M, Erhan B, Akkoc Y, et al: An evaluation of bladder emptying strategies and the impact of demographic and scientific elements on spontaneous voiding frequency in stroke patients, Neurol Sci 34:729�734, 2013. Fagan M, Maehlen M, Lindbaek M, et al: Antibiotic prescribing in nursing houses in an space with low prevalence of antibiotic resistance: compliance with nationwide guidelines, Scan J Prim Health Care 30:10�15, 2012. Garre-Olmo J, Planas-Pujol X, Lopez-Pousa S, et al: Prevalence and danger components of suspected elder abuse subtypes in people aged seventy five and older, J Am Geriatr Soc 57:815�822, 2009. Gesenberg A, Sintermann R: Management of benign prostatic hyperplasia in high risk sufferers: long-term expertise with the Memotherm stent, J Urol a hundred and sixty:72�76, 1998. Gooren L, Lips P: Conjectures concerning cross-sex hormone remedy of getting older transsexual individuals, J Sex Med eleven:2012�2019, 2014. Gotoh M, Matsukawa Y, Yoshikawa Y, et al: Impact of urinary incontinence on the psychological burden of family caregivers, Neurourol Urodyn 28:492�496, 2009. Federal Interagency Forum on Aging-Related Statistics: Older Americans 2012: Key indicators of well-being. Fontana L, Addante F, Copetti M, et al: Identification of a metabolic signature for multidimensional impairment and mortality danger in hospitalized older sufferers, Aging Cell 12:459�466, 2013. Fox C, Smith T, Maidment I, et al: Effect of medicines with anti-cholinergic properties on cognitive perform, delirium, bodily function and mortality: a scientific review, Age Ageing 43:604�615, 2014. Fraisse T, Crouzet J, Lachaud L, et al: Candiduria in those over eighty five years old: a retrospective examine of 73 patients, Intern Med 50:1935�1940, 2011. Frost M, Wraae K, Gudex C, et al: Chronic diseases in elderly males: underreporting and underdiagnosis, Age Ageing 41:177�183, 2012. Fung C, Pandya C, Guancial E, et al: Impact of bladder most cancers on health associated high quality of life in 1,476 older Americans: a cross-sectional research, J Urol 192:690�695, 2014. Galizia G, Langellotto A, Cacciatore F, et al: Association between nocturia and falls-related long-term mortality risk within the aged, J Am Med Dir Assoc 13:640�644, 2012. Guillotreau J, Miocinovic R, Game X, et al: Outcomes of laparoscopic and robotic radical cystectomy within the aged patients, Urology seventy nine:585�590, 2012. Haruta H, Sakakibara R, Ogata T, et al: Inhibitory management task is decreased in vascular incontinence sufferers, Clin Auton Res 23:85�89, 2013. Hasegawa J, Kuzuya M, Iguchi A: Urinary incontinence and behavioral symptoms are unbiased risk elements for recurrent and injurious falls, respectively, amongst residents in long-term care facilities, Arch Gerontol Geriatr 50:77�81, 2010. Hashimoto M, Imamura T, Tanimukai S, et al: Urinary incontinence: an unrecognised opposed effect with donepezil, Lancet 356:568, 2000. Hill-Brown S: Reduction of strain ulcer incidence in the residence healthcare setting, Home Healthc Nurse 29:311�325, 2011. Hoshiyama F, Hirayama A, Tanaka M, et al: the influence of obstructive sleep apnea syndrome on nocturnal urine production in older males with nocturia, Urology 84:892�897, 2014. Ikeda Y, Nakagawa H, Ohmori-Matsuda K, et al: Risk components for overactive bladder within the aged inhabitants: a community-based examine with face-to-face interview, Int J Urol 18:212�218, 2011. Iwatsubo E, Suzuki M, Igawa Y, et al: Individually tailor-made ultrasound-assisted prompted voiding for institutionalized older adults with urinary incontinence, Int J Urol 21:1253�1257, 2014. Kates M, Badalato G, Pitman M, et al: Persistent overuse of radical nephrectomy in the elderly, Urology seventy eight:555�559, 2011. Kim H, Yoshida H, Hu X, et al: Association between self-reported urinary incontinence and musculoskeletal circumstances in community-dwelling aged girls: a cross-sectional research, Neurourol Urodyn 34:322�326, 2015. Klauser A, Frauscher F, Strasser H, et al: Age-related rhabdosphincter function in female urinary stress incontinence: evaluation of intraurethral sonography, J Ultrasound Med 23:631�637, 2004. Kohjimoto Y, Iba A, Shintani Y, et al: Impact of patient age on outcome following bladder-preserving remedy for non-muscle-invasive bladder cancer, World J Urol 28:425�430, 2010. Kojima Y, Takahashi N, Haga N, et al: Urinary incontinence after robot-assisted radical prostatectomy: pathophysiology and intraoperative strategies to enhance surgical end result, Int J Urol 20:1052�1063, 2013. Jaul E: Assessment and administration of pressure ulcers in the aged: present strategies, Drugs Aging 27:311�325, 2010. Jazzar U, Yong S, Klaassen Z, et al: Impact of psychiatric illness on decreased survival in aged sufferers with bladder most cancers within the United States, Cancer 124:3127�3135, 2018. Johnell K, Fastbom J: Concurrent use of anticholinergic medicine and cholinesterase inhibitors: register-based study of over 700,000 aged sufferers, Drugs Aging 25:871�877, 2008. Joseph B, Pandit V, Zangbar B, et al: Validating trauma-specific frailty index for geriatric trauma sufferers: a potential analysis, J Am Coll Surg 219:10�18, 2014. Justo D, Arbel Y, Mulat B, et al: Sexual exercise and erectile dysfunction in elderly men with angiographically documented coronary artery disease, Int J Impot Res 22:40�44, 2010. Juthani-Mehta M: Asymptomatic bacteriuria and urinary tract an infection in older adults, Clin Geriatr Med 23:585�594, 2007. Juthani-Mehta M, Quagliarello V, Perrelli E, et al: Clinical options to establish urinary tract an infection in nursing home residents: a cohort research, J Am Geriatr Soc fifty seven:963�970, 2009. Juthani-Mehta M, Tinetti M, Perrelli E, et al: Diagnostic accuracy of standards for urinary tract an infection in a cohort of nursing house residents, J Am Geriatr Soc 55:1072�1077, 2007. Kafri R, Kodesh A, Shames J, et al: Depressive symptoms and remedy of women with urgency urinary incontinence, Int Urogynecol J 24:1953�1959, 2013. Kamdar A, Yahya A, Thangaraj L: Retrospective observational examine of the incidence of short-term indwelling urinary catheters in elderly patients with neck of femur fractures, Geriatr Gerontol Int 9:131�134, 2009. K�rnig M, Br�hlmann E, G�nthert A, et al: Intra-, peri- and postoperative complications in pelvic organ prolapse surgical procedure in geriatric girls, Eur J Obstet Gynecol Reprod Biol 224:142�145, 2018. Koskim�ki J, Shiri R, Tammela T, et al: Regular intercourse protects in opposition to erectile dysfunction: Tampere Aging Male Urologic Study, Am J Med 121:592�596, 2008. Kouloulias V, Tolia M, Kolliarakis N, et al: Evaluation of acute toxicity and signs palliation in a hypofractionated weekly schedule of exterior radiotherapy for aged patients with muscular invasive bladder most cancers, Int Braz J Urol 39:77�82, 2013. K�ves B, Cai T, Veeratterapillay R, et al: Benefits and harms of remedy of asymptomatic bacteriuria: a systematic evaluation and meta-analysis by the European Association Of Urology Urological Infection Guidelines Panel, Eur Urol 72:865�868, 2017. Kovindha A, Wattanapan P, Dejpratham P, et al: Prevalence of incontinence in patients after stroke during rehabilitation: a multi-centre study, J Rehabil Med forty one:489�491, 2009. Koyama M, Steinman K, Ensrud T, et al: Long-term cognitive and functional results of doubtless inappropriate medicines in older ladies, J Gerontol A Biol Sci Med Sci sixty nine:423�429, 2014. Kurihara M, Murakami G, Kajiwara M, et al: Lack of the complete round rhabdosphincter and a distinct round clean muscle layer across the proximal urethra in aged Japanese ladies: an anatomical research, Int Urogynecol J Pelvic Floor Dysfunct 15:85�94, 2004. Kurtal H, Schwenger V, Azzaro M, et al: Clinical worth of automated reporting of estimated glomerular filtration rate in geriatrics, Gerontology 55:288�295, 2009. Landi F, Cesari M, Russo A, et al: Benzodiazepines and the danger of urinary incontinence in frail older individuals living in the neighborhood, Clin Pharmacol Ther 72(6):729�734, 2002. Drugs for the prevention of postoperative urinary retention in adults (Protocol), Cochrane Database Syst Rev (10):Art. Lewicky-Gaupp C, Hamilton Q, Ashton-Miller J, et al: Anal sphincter structure and function relationships in growing older and fecal incontinence, Am J Obstet Gynecol 200(559):e551�e555, 2009. Liberman D, Lughezzani G, Sun M, et al: Perioperative mortality is considerably higher in septuagenarian and octogenarian sufferers handled with radical cystectomy for urothelial carcinoma of the bladder, Urology seventy seven:660�666, 2011. Lightner D, Calvosa C, Andersen R, et al: A new injectable bulking agent for remedy of stress urinary incontinence: outcomes of a multicenter, randomized, managed, double-blind research of Durasphere, Urology fifty eight:12�15, 2001.






