Protonix
Protonix
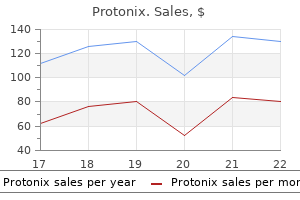
Protonix dosages: 40 mg, 20 mg
Protonix packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

The massive thought: iron-dependent irritation in venous illness and proposed parallels in a number of sclerosis chronic gastritis biopsy protonix 40 mg cheap without prescription. A prospective open-label examine of endovascular therapy of chronic cerebrospinal venous insufficiency gastritis diet vegetables protonix 40 mg buy discount line. Structural dynamics of oligodendrocyte lysis by perforin in tradition: relevance to multiple sclerosis diet of gastritis protonix 40 mg order with visa. Reactive astrocytes in continual lively lesions of a quantity of sclerosis categorical costimulatory molecules B7-1 and B7-2. Relapsing demyelinating disease affecting both the central and peripheral nervous techniques. Persistent reflection underlies ectopic activity in multiple sclerosis: a numerical research. The relative number of macrophages/ microglia expressing macrophage colonystimulating issue and its receptor decreases in a quantity of sclerosis lesions. Multiple sclerosis: altered glutamate homeostasis in lesions correlates with oligodendrocyte and axonal damage. Water diffusion is elevated in widespread areas of normal-appearing white matter in multiple sclerosis and correlates with diffusion in focal lesions. Normal-appearing white matter in a number of sclerosis has heterogeneous, diffusely extended T2. Human oligodendrocyte precursor cells in vitro: phenotypic evaluation and differential response to development components. Multiple Sclerosis; current and emerging diseasemodifying therapies and therapy strategies. The emerging relationship between neuromyelitis optica and systemic rheumatologic autoimmune illness. At any stage, this method may be affected by quite so much of multifocal and systemic disorders. Rarely, the axonal degenerative process begins proximally and progresses downstream. Axonopathies can also be focal; disorders that instantly have an effect on the Schwann cell or myelin result in major segmental demyelination. It is this organic interdependence of the ganglion cell, the axon or dendrites, the Schwann cell and the supporting connective vascular tissue that explains the stereotyped response of the nerve fibre to a selection of totally different pathological insults. In many circumstances, sensory signs and signs are inclined to dominate initially, as a result of the longest axons are these supplying the toes and toes, whereas motor involvement necessitates progression of the illness to involvement of more proximal segments of nerve serving major muscle groups. Dysfunction of huge fibres produces deficits in vibration and joint place sensation, and impairment of deep tendon reflexes that are transmitted by 1A afferent sensory axons. There is a slender vary of diagnoses for polyneuropathies affecting small fibres (Table 24. The diagnosis of pure motor neuropathy is fraught with problem due to the overlapping scientific features of peripheral nerve motor dysfunction with illnesses of the decrease motor neuron. Such circumstances could end in scientific and electrophysiological modifications of their own that hinder attempts to arrive at a analysis. Furthermore, sufferers with generalized peripheral neuropathy appear more susceptible to compression neuropathies. The most common sample is a length-dependent course of in which the distal elements of extremities are affected first, symmetrically, with development evolving from toes to ankles and from fingertips to wrist, and into the classic glove�stocking pattern. Paraproteinaemic neuropathy and a few metabolic circumstances can also have a gradual, indolent course. Neuropathies that evolve over a few years without inflicting major disability usually elude diagnosis despite in depth testing (cryptogenic neuropathies) and are notably frequent in aged patients. Because some subcutaneous nerves contain nerve fibres that are far removed from their father or mother ganglion cell (the separation could exceed 1 metre in nerves to the decrease limb), any estimate of illness affecting the perikaryon is a prediction made by inference of abnormalities in distal dendrites and axons. When compared with the dimension of the cell body, axons and dendrites in peripheral nerve may represent the most important component of the entire mass of the neuron; however, only small segments of nerve bundles are visualized in a nerve biopsy. For instance, in a big series of subcutaneous nerve biopsies performed over a 33-year period and comprising practically one thousand consecutive cases on the University of Toronto, a specific prognosis was established only in about 29 per cent of instances. This syndrome of small-fibre neuropathy is a source of frustration for the clinician, because the seek for a specific diagnosis with bodily examination, electrodiagnostic research and even subcutaneous nerve biopsy usually ends in an absence of objective findings. The differential analysis of predominantly smallfibre neuropathy is proscribed (Table 24. The fine innervation of the human epidermis was initially described in 1868 by Paul Langerhans, then a medical pupil. They estimated the number of nerve endings per unit area and found a variety of individual variation and a rostral to caudal gradient of innervation. Combined with the advances supplied by the confocal microscope, which permits the three-dimensional reconstruction of thick sections of pores and skin, this stimulated analysis into the cutaneous innervation and the examine of patients with small-fibre neuropathies. Additional immunolabelling for different neuropeptides allows assessment of the innervation of sweat glands, arterioles, papilla and hair follicles. One of the restrictions of this system is the necessity to have an adequate financial institution of management specimens from the completely different parts of the body to correlate with the biopsy sites used. In addition, the normal sample has to be obtained from age-matched controls that have been subjected to rigorous neurological and electrophysiological 24 1416 Chapter 24 Diseases of Peripheral Nerves studies to rule out subclinical disease. Furthermore, the distribution density of epidermal nerve fibres differs in various parts of the physique: studies have proven the density of epidermal fibres to be lower in males and to decrease with age (range 4. Contained within the perineurium is the endoneurium, consisting of a collagenous matrix housing the axons, Schwann cells, fibroblasts, macrophages, mast cells and capillaries. Normal peripheral nerves consist of a bundle of fascicles encased in a fibrovascular stroma termed the epineurium. Individual peripheral and autonomic nerve fascicles are further ensheathed by perineurium, a specialised structure the epineurium the epineurium consists of massed collagen fibrils (types 1 and 3) interspersed with occasional elastin fibres, fibroblasts, mast cells, and the small arterial and venous blood vessels that provide the capillary plexus of the underlying nerve. Superficially, the epineurium merges with the encircling areolar connective tissue of the deep fascia, and on its deep surface with the outermost layer of the perineurium. The number of layers is highest proximally, progressively diminishing to a single layer on the finest distal cutaneous and intramuscular nerve branches. In larger nerves, septa composed of two or three layers of perineurial cells arising from the internal side of the sheath could subdivide particular person funiculi into Peri Endo Epi 24. A, axon; Endo, endoneurium; Epi, epineurium; F, fibroblast; P, perineurium; S, Schwann cell. The connective tissue between the layers exhibits collagen fibrils (C) and elaunin (e). Blood vessels penetrating the perineurium to supply the endoneurial capillary plexus also carry sleeves of perineurial cells with them into the endoneurium for brief distances. In sections, the person perineurial cells seem as skinny sheets of cytoplasm, often no extra than 0. Both faces of the perineurial cells are coated by basal lamina, which may turn into thickened in comparison with the basal laminae of other cells, even in quite young topics, and to which the cell membrane could additionally be anchored by scattered hemi-desmosomes. The connective tissue between these layers of cells consists of collagen fibrils (40�80 nm) and occasional elastic fibrils. At their margins, the individual perineurial cells overlap and interdigitate and are linked by tight junctions between their apposed membranes. Note plentiful collagen fibrils (C) within the matrix operating in parallel with the axons. In addition, every nerve fibre is surrounded immediately outside the Schwann cell basal lamina by a skinny sleeve of a lot finer, extra irregularly disposed reticulin fibres. These are angular cells missing a basal lamina that lie free between the endoneurial collagen fibrils. Other cells which may be discovered within the endoneurium are mast cells and macrophages. Resident macrophages are a normal constituent of the endoneurium, contributing some 2�5 per cent of the inhabitants. They are located predominantly near blood vessels or the inner side of the perineurium, and they are probably to have a dendritic morphology, with their processes oriented alongside the longitudinal axis of the nerve. Injury to , or illness of, peripheral nerves results in a speedy inflow of an additional haematogenously derived inhabitants of macrophages at the web site of the lesion, the trigger for recruitment being the presence of degenerating axons.
Furthermore gastritis detox diet discount protonix 40 mg on-line, in this regard gastritis y colitis nerviosa sintomas protonix 20 mg discount with visa, corticosteroid-induced alterations within the variety of intracerebral T-cells also have to gastritis diet ���� protonix 40 mg cheap on line be thought of. These efforts, nonetheless, were largely disappointing because in biopsies, frozen tissue was both not available or not appropriate for analysis because of infectivity, whereas autopsy-derived tissue was often too degraded for molecular studies. Thus, compared to immunocompetent patients, knowledge of the biology is rather limited. Combined chemoradiotherapy achieved full response charges of as much as 87 per cent with a median progression-free survival of up to forty months. However, unfortunately, chemotherapy followed by radiotherapy triggered delayed extreme neurotoxicity, which clinically manifested as extreme neurological impairment, extreme cognitive dysfunction, dementia, and dying, notably in older patients (>60 years). Macroscopy demonstrated white matter damage with diffuse pallor sparing the arcuate fibres and white matter necrosis. Clinically, neurological signs could increase the differential diagnosis of cerebral vasculitis, dementing disorders and even Creutzfeldt�Jakob disease. Macroscopically, acute or old ischaemic infarcts, regularly scattered as multiple infarcts, necrosis or bleeding, including purpura cerebri with a number of haemorrhages, may be seen. Occluded vessels may be recanalized and associated with a number of current and older anaemic infarcts. Depending on the topography of the lesion, neurological symptoms are highly variable and embody hemiparesis, ataxia, cranial nerve palsies and confusional states. Blood vessel partitions are infiltrated and surrounded by mature leukocytic infiltrates composed of lymphocytes, plasma cells, histiocytes and immunoblasts. Because of the angiotropism of the lymphoma cells, vasculitis, fibrinoid blood vessel necrosis and infarct-like necrosis are distinguished. Angiotropic lymphoma (Intravascular lymphoma) Typically, this tumour manifests in adult sufferers (median, 67 years; range, 13�85 years), affecting both sexes equally. Diffuse and focal neurological indicators occurred in eighty two and seventy two per cent of sufferers, respectively. Clinically, multifocal leukoencephalopathy with motor dysfunction, reminiscence loss, confusion and coma has been reported. Morphologically, the tumour cells correspond to small lymphocytes, plasmacytoid lymphocytes and plasma cells. Most cells show floor expression of Ig; plasmacytic cells largely categorical IgM, occasionally IgG, and solely seldom IgA. Patients develop diverse, nonspecific symptoms together with headache, psychological modifications suggestive of dementia, seizures, sensory deficits, cerebellar signs and cranial nerve dysfunction. Overall, neurological signs elevate the differential diagnosis of viral encephalitis or toxicmetabolic encephalopathies. The tumour Plasmacytoma Plasmacytoma incessantly includes the bone of the skull and the vertebral column, where it causes lytic lesions, often a quantity of in quantity. Neurological symptoms (paraplegia) occur when vertebral lesions progress to spinal twine compression. Extranodal marginal Zone lymphoma Twelve per cent of extranodal marginal zone lymphomas arise in the ocular adnexa. Here, the orbit is the most frequent site of origin accounting for approximately forty per cent of circumstances. Exceptionally, marginal zone lymphoma has been reported to infiltrate the basal ganglia and temporal lobe without dural involvement. Acute onset of symptoms raising the differential analysis of subdural hematoma has additionally been noticed. Morphologically, tumour cells contain small- to mediumsized nuclei with pale cytoplasm, resembling centrocytes. A few bigger cells resembling immunoblasts or centroblasts can also be intermingled. Centrocytes similar to small- to mediumsized cells with cleaved nuclei and slim cytoplasm usually dominate the tumour. Centroblasts are characterised by an increased dimension and harbour spherical to oval, giant nuclei with outstanding nucleoli and scant, basophilic cytoplasm. Morphology reveals cells resembling immunoblasts with giant nuclei, prominent nucleoli and ample cytoplasm. Mitotic and proliferative exercise is excessive with a Ki67 staining index usually exceeding 90 per cent of the tumour cells. Morphologically, the tumour cells are monomorphic and of medium measurement with round nuclei harbouring multiple nucleoli positioned paracentrally and a basophilic cytoplasm incorporating lipid vacuoles. Mitoses are frequent, and, correspondingly, proliferative exercise is very excessive with nearly all tumour cells expressing the Ki-67 antigen. Tumour cells specific surface IgM/IgD with evidence for light chain restriction with a extra frequent expression of the than the light chain. Tumours are in contact with the dura typically, however location within the brain parenchyma has additionally been reported. Histologically, traditional multinucleated Reed�Sternberg cells, characterised by massive nuclei with conspicuous nucleoli and a distinguished nuclear membrane, as properly as a barely basophilic cytoplasm, are embedded in a background of an inflammatory infiltrate consisting of lymphocytes, histiocytes and eosinophils. Hodgkin and Reed�Sternberg cells are latently contaminated by Epstein�Barr virus in about forty per cent of sufferers. A median of age 60 years with a variety of 3�84 years and a male to feminine ratio of 2�3:1 have been reported. In the brain, the majority of circumstances reported manifested within the supratentorial space affecting the cerebral hemispheres (64 per cent), basal ganglia (11 per cent) and corpus callosum (13 per cent). Space-occupying mass lesions with greyish to yellow colour present ill-defined margins and will comprise haemorrhage and necrosis. Definite prognosis depends on the histopathological identification of malignant T cells. Tumour cells correspond to atypical lymphoid cells of small or medium measurement with nuclear pleomorphism. In addition, corticosteroidinduced regression of malignant B cells could mimic T-cell lymphoma. Such cases may also present remarkably elevated proliferative activity (>30 per cent). Proliferative exercise is usually high, and greater than 70 per cent of the tumour cells may specific the Ki-67 antigen. Large cells with eccentric, horseshoeor kidney-shaped nuclei with an eosinophilic perinuclear area are characteristic. Because sufferers with leukaemia could have coagulation disturbances, bleeding in an atypical location ought to increase the suspicion of tumourous bleeding and foster a cautious search for blasts inside the hematoma. Morphologically, myeloblasts have scant cytoplasmic rims, massive nuclei and outstanding nucleoli and present vigorous mitotic activity. Meningeal chloroma (granulocytic sarcoma) in acute lymphoblastic leukemia mimicking a falx meningioma. Clinical relevance of flow cytometric immunophenotyping of the cerebrospinal fluid in sufferers with diffuse large B-cell lymphoma. Primary central nervous system posttransplantation lymphoproliferative disorder: an International Primary Central Nervous System Lymphoma Collaborative Group Report. Primary brain and central nervous system tumors identified within the United States in 2004� 2008. Changing pattern of primary cerebral lymphoma within the highly energetic antiretroviral therapy period. Primary central nervous system lymphoma: age and efficiency standing are more important than therapy modality. Modern ideas within the biology, analysis, differential analysis and remedy of primary central nervous system lymphoma. Multicenter evaluation of eighty strong organ transplantation recipients with post-transplantation lymphoproliferative disease: outcomes and prognostic factors within the fashionable period. Aberrant methylation in the promoter area of the reduced folate carrier gene is a possible mechanism of resistance to methotrexate in primary central nervous system lymphomas. Leptomeningeal involvement in continual lymphocytic leukemia identified by polymerase chain response in saved slides: a case report.
Differential expression of extracellular matrix-related genes in uncommon variants of meningioma gastritis keeps coming back protonix 40 mg purchase overnight delivery. Intracranial meningiomas: correlation of peritumoral edema and psychiatric disturbances gastritis blog generic 20 mg protonix with mastercard. Vascular endothelial development issue gastritis main symptoms generic protonix 20 mg with visa, hepatocyte growth factor/scatter factor, primary fibroblast development issue, and placenta development factor in human meningiomas and their relation to angiogenesis and malignancy. IgG4-related meningeal illness: clinicopathological features and proposal for diagnostic standards. An analysis of the magnetic resonance imaging and pathology of intracal lymphoplasmacyte-rich meningioma. Benign tumors from the human nervous system express high levels of survivin and are immune to spontaneous and radiation-induced apoptosis. Multiple meningiomas: investigating the molecular basis of sporadic and familial forms. Clear cell meningioma with histologically aggressive appearance and clinically aggressive habits: a case report. Fibroblast progress factor receptor-3 expression in meningiomas with stimulation of proliferation by the phosphoinositide three kinase-Akt pathway. Bone morphogenetic protein 4 and its receptors are expressed within the leptomeninges and meningiomas and sign by way of the Smad pathway. Evidence for phosphatidylinositol 3-kinase-Akt-p7S6K pathway activation and transduction of mitogenic alerts by platelet-derived growth consider meningioma cells. Factors affecting operative and excess long-term mortality in 935 sufferers with intracranial meningioma. Different activation of mitogen-activated protein kinase and Akt signaling is related to aggressive phenotype of human meningiomas. Antitumor exercise of the growth hormone receptor antagonist pegvisomant towards human meningiomas in nude mice. Factors affecting peritumoral mind edema in meningioma: particular histological subtypes with prominently intensive edema. The function of matrix metalloproteinases and tissue inhibitors of matrix metalloproteinase in microcystic meningiomas. A position for chromosome 9p21 deletions in the malignant progression of meningiomas and the prognosis of anaplastic meningiomas. Cytogenetic analysis of aggressive meningiomas: possible diagnostic and prognostic implications. Meningothelial hyperplasia: an in depth clinicopathologic, immunohistochemical and genetic study of eleven circumstances. Peyre M, Stemmer-Rachamimov A, Clermont-Taranchon E, Quentin S, ElTaraya N, Walczak C, et al. Molecular genetics of meningiomas: a systematic review of the present literature and potential basis for future remedy paradigms. History of head trauma and danger of intracranial meningioma: populationbased case-control research. Anaplastic meningioma versus meningeal hemangiopericytoma: immunohistochemical and genetic markers. Expression of matrix metalloproteinases, their inhibitors, and urokinase plasminogen activator in human meningiomas. Anterior visual pathway meningiomas primarily resected between 1978 and 1988: the Mayo Clinic Rochester experience. Unbalanced translocation t(1;3)(p12�13;q11) in meningiomas because the distinctive feature of chordoid differentiation. Clinical options and immunohistochemical expression levels of androgen, estrogen, progesterone and Ki-67 receptors in relationship with grosstotal resected meningiomas relapse. Pediatric meningiomas within the Netherlands 1974�2010: a descriptive epidemiological case examine. Molecular characterization of human meningiomas by gene expression profiling utilizing highdensity oligonucleotide microarrays. Analysis of genomic alterations in benign, atypical, and anaplastic meningiomas: towards a genetic mannequin of meningioma development. Quantitative evaluation of neurofibromatosis type 2 gene transcripts in meningiomas supports the idea of distinct molecular variants. Progesteronereceptor index in meningiomas: correlation with clinico-pathological parameters and evaluation of the literature. Microarray-based gene expression profiling of benign, atypical and anaplastic meningiomas identifies novel genes one hundred fifty five. Lipomatous meningioma: a clinicopathologic examine of 18 cases with particular reference to the issue of metaplasia. Immunohistochemical willpower of 5 somatostatin receptors in meningioma reveals frequent overexpression of somatostatin receptor subtype sst2A. Intranuclear inclusions of meningioma related to irregular cytoskeletal protein expression. Peritumoral brain edema related to meningioma: influence of vascular endothelial progress factor expression and vascular blood supply. Meningioma: a cytogenetic model of a posh benign human tumor, including data on 394 karyotyped cases. Clinicopathological analysis of rhabdoid meningiomas: report of 12 instances and a scientific review of the literature. As a basic rule, they share histologic, immunohistochemical and molecular alterations with their gentle tissue and bone counterparts. Showing neither true meningothelial nor pericytic differentiation, its histogenesis stays a mystery. A reticulin-rich network surrounding particular person tumour cells is often present, though with vital intertumoural and intratumoural variability. Claudin-1 appears to be a more particular, though not particularly sensitive, marker for meningiomas. The tumour accommodates multiple signal voids, indicating the highly vascular nature of the lesion. Up to 10�15 per cent present malignant behaviour with native recurrence, cerebrospinal fluid dissemination or metastatic disease. Meningeal sarcomas happen preferentially in youthful sufferers, including youngsters, and without obvious intercourse predilections. Most are clearly related to the dura or leptomeninges, and the base of the skull is a common sight. Historically, only some variants of meningeal sarcoma have been recognized, with the descriptive names of fibrosarcomas, spindle cell sarcomas and polymorphic cell sarcomas. At the low grade finish of the spectrum are cavernous haemangiomas, comprised of thin-walled gaping vascular channels lined by a single layer of bland endothelium. Most regularly presenting with seizures as a supratentorial intraparenchymal lesion with a surrounding rim of microhaemorrhage and hemosiderin deposition, cavernous haemangioma has on uncommon occasions been encountered arising from the dura on the ground of the center cranial fossa. Similar to its extracranial counterpart, full resection affords a beneficial consequence. The majority arise in adults and are dural based mostly, although occasional intraparenchymal examples have been encountered. Occasional pleomorphic cells, together with multinucleate types, or focal necrosis are seen. The evaluate by Gaspar and colleagues demonstrated the propensity of main intracranial fibrosarcoma to present native and distant recurrence, meningeal seeding and systemic metastases. Pleomorphic sarcomas, not otherwise specified, are equivalent to their counterparts in delicate tissues, containing a storiform pattern of spindle-shaped cells interspersed with massive pleomorphic, often lipidized cells. Though extra frequently arising within the surrounding bony constructions, circumstances inside the craniospinal vault have been encountered. Once skeletal muscle differentiation is documented, a primitive neuroectodermal tumour exhibiting focal rhabdomyoblastic differentiation. In addition, leiomyosarcomas are extra cellular with architectural disarray, brisk mitotic exercise and necrosis. Correct analysis rests on an acceptable immunoprofile, such as clean muscle actin expression or filaments with dense our bodies on electron microscopy. Intracranial Ewing sarcoma/"peripheral" primitive neuroectodermal tumor of dural origin with molecular genetic confirmation.
The myonuclei round neuromuscular junctions are specialised and have a job in the transcription of the precise proteins of the neuromuscular junction gastritis reddit protonix 40 mg discount fast delivery. With the Verhoeff� van Gieson stain gastritis beans purchase protonix 20 mg on-line, individual axons and their myelin sheaths stain black and may be readily visualized; with the Gomori trichrome stain gastritis symptoms pdf buy generic protonix 20 mg, the myelin of particular person axons stains red. The fibre type profile varies between muscles and even across different areas of the identical muscle. The total properties of any given muscle end result largely from the proportion of its completely different fibre sorts, that are influenced by innervation/neuromuscular exercise, exercise/training, mechanical loading/unloading, hormones and ageing. Alterations in fibre sort profile can also be influenced by varied pathological processes (see General Histological and Histochemical Abnormalities, p. The high oxidative metabolism of kind 1 fibres is also mirrored in the next lipid content, which can be demonstrated with oil red O, Sudan black and Nile pink dyes. Three fibre varieties can thus be recognized in normal muscle (types 1, 2A and 2B), with an extra 25. However, the identification of those fibres is now 1530 (a) Chapter 25 Diseases of Skeletal Muscle (a) 2B 1 2A 2C (b) (b) 2B 1 2A 2C (c) 2B 25. In practice, the most important diagnostic distinction is between type 1 and all kind 2 fibres (slow versus fast myosin). Studies with antibodies specific to quick 2X myosin are restricted, and it has not been extensively studied in pathological samples. In common, type 1 fibres have wider Z-lines and extra mitochondria and lipid, however a much less in depth sarcoplasmic reticulum, T-tubule system, triads and glycogen. The appearance of the M-line can also be attribute of the fibre type, muscle and species from which the part has been taken. Ultrastructural variations are less distinct in human muscle than in different species, but the Z-line and M-line, both alone or in combination, could be good indicators of fibre type in the human tibialis anterior, where type 1 fibres had been shown to have broader Z-lines and five robust M-bridge lines; sort 2A fibres to have intermediate Z-lines, three sturdy M-bridge traces and two weak M-bridge lines; and sort 2B fibres to have narrow Z-lines and three strong M-bridge strains, with the 2 outer ones being very weak or absent. Fibre nuclei align with their longitudinal axes parallel to that of the fibre, and in longitudinal section they are often seen to be elliptical and display dense peripheral heterochromatin, along with a prominent nucleolus and finely stippled nucleoplasm. A double nuclear membrane surrounds the nucleus, the outer of which is steady with the endoplasmic reticulum. The nuclear membrane is associated with essential proteins, including emerin, lamin A/C and nesprins, which can be faulty in neuromuscular disorders (see Emery�Dreifuss Muscular Dystrophy, p. Emerin is a element of the inner nuclear membrane itself, whereas lamin A/C, along with other lamins and associated proteins, is localized to the nuclear lamina beneath the nuclear membrane. All nuclei are basophilic, stain blue with haematoxylin after an alkaline rinse, and normally stain red with the acid pH of the Gomori trichrome stain. The nuclei of the syncytial grownup muscle fibres are post-mitotic and unable to bear division. Muscle fibre number in mammals is generally determined prenatally or soon after (up to four months in humans), and any improve in muscle measurement is due to increases in the size, not quantity, of the individual fibres. Postnatally, fibre dimension is regulated by both the variety of nuclei integrated into each fibre and the volume of cytoplasm that each nucleus helps, which varies between completely different fibre types. The primary source of all new nuclei added to the fibre throughout progress and regeneration is the satellite cell population, where stem cell activity is assumed to reside. Muscle at birth incorporates a excessive proportion of satellite tv for pc cells � sometimes 30 per cent � however this decreases to around 5 per cent in adult life. Ultrastructurally, satellite cells have nuclei with dense peripheral heterochromatin and a small volume of cytoplasm that accommodates few organelles, free ribosomes, rough endoplasmic reticulum, glycogen, microtubules and intermediate filaments. Most muscle tissue, aside from some craniofacial and oesophageal muscles, are derived from the somites. Genetargeting experiments in the mouse outline a transcriptional hierarchy in which the paired-domain transcription elements 25 25. These myotubes have giant central nuclei with a prominent nucleolus, and scattered myofibrils. Early major myotubes are initially clustered inside a standard basal lamina, however as differentiation continues every becomes surrounded by its own basal lamina. Secondary myotubes come up from successive waves of fusion of post-mitotic myoblasts, alongside the surface of the first myotubes. These initially type within the neighborhood of innervation websites on the primary myotube, and early secondary myotubes are at first encased within the identical basal lamina as the father or mother main myotube. With increased maturation, these secondary myotubes separate and attain their own basal lamina. Fibre typing, significantly with antibodies to myosin isoforms, could be observed from about 10�12 weeks of gestation in human fetal quadriceps. Myosin heavy chain isoforms are expressed sequentially throughout improvement and are influenced by each innervation and hormones. Primary myotubes are innervated by pioneering axons at an early part of myogenesis, and most specific sluggish myosin and are destined to turn into gradual, kind 1 fibres. It has been proposed that these represent the fundamental motor models of the growing neuromuscular system and are responsible for early slow movements. Secondary myotubes, nonetheless, are hybrid fibres and may express various mixtures of fetal/neonatal, quick and sluggish myosin. These turn out to be organized into massive, quick motor models later in development, eclipsing the unique slow response. In human fetal quadriceps muscular tissues, a population of very small myotubes � secondary myotubes, typically referred to as tertiary myotubes � seems at about 12�13 weeks of gestation. At start, a selection of fibres stain histochemically as 2C fibres and coexpress fetal myosin with quick or sluggish myosin. In our experience, many fibres from neonates specific fetal/neonatal myosin; nevertheless, by 3�4 months of age very few may be seen, and some may stay up to 1 12 months of age. During the neonatal interval, some fibres with a very large diameter stain intensely with most histological stains and have properties of type 1 fibres. This circulate of ions induces a voltage change, which ends up in the opening of voltage-gated sodium channels within the plasma membrane of the sarcolemma, adopted by depolarization. This allows a large inflow of constructive ions, resulting in depolarization of the postsynaptic membrane and muscle fibre. Cholinesterase is secreted by the muscle cell and is anchored to the basal lamina that lies between the nerve terminal and the muscle end plate. The calcium is released from the lateral sacs of sarcoplasmic reticulum adjacent to the T-tubules, and muscle contraction is initiated inside milliseconds of depolarization of the motor end plate. Both genetic defects of various proteins that type the neuromuscular junction and acquired autoimmune variants are identified, (see Myasthenic Syndromes, p. According to the sliding filament mannequin of muscle contraction, shortening of the sarcomere is achieved via the action of (thin) actin filaments sliding (or being pulled) along the (thick) myosin filaments. Few are pathognomonic of a selected disease, however a mixture current in a pattern, and assessed in the context of the scientific features, often leads to identification of the kind of disorder, if not an correct prognosis. Multidisciplinary meetings between the pathologist and clinicians play a vital half in directing further investigations. Every pathologist tends to have a favoured panel of strategies to apply to a muscle biopsy, neuromuscular transmission and Muscle contraction Neuromuscular transmission is the process by which an action potential generated in motor neurons passes down General Histological and Histochemical Abnormalities field 25. More details in relation to specific issues and gene defects are described in the applicable sections. Sample handling and freezing technique, nonetheless, can affect the shape and degree of separation of the person fibres. Fibre sizes improve with age, and knowledge of this normal variation is important. It is usually enough to measure the smallest and largest fibres in a sample in order to acquire an approximate range of fibre sizes and to point out whether this is appropriate for age and intercourse. Ideally, every pathology division ought to establish its own vary of normal sizes, but obtaining samples from unequivocally regular individuals is ethically problematic, and lots of workers rely on printed data. Fibre measurement is affected by a number of elements, together with innervation, progress factors. Excessive load on a muscle ends in an increase in fibre size (hypertrophy), whereas disuse and denervation cause a decrease in size (atrophy). Longitudinal splitting and branching of fibres occur under sure pathological circumstances and contribute to the presence in cross-section of small fibres. Atrophy or hypertrophy of both fibre sorts occurs in most myopathic issues, however in some cases it may specifically affect one fibre type.
Prevalence of glioblastoma multiforme in subjects with prior therapeutic radiation chronic gastritis what to eat order protonix 20 mg without prescription. Maternal smoking throughout pregnancy and the chance of childhood mind tumors: a meta-analysis of 6566 topics from twelve epidemiological studies eosinophilic gastritis diet discount protonix 20 mg free shipping. Dietary cured meat and the chance of grownup glioma: a meta-analysis of 9 observational studies chronic gastritis medicine cheap protonix 20 mg without prescription. Genetically engineered mouse models of mind most cancers and the promise of preclinical testing. The changing epidemiology of paediatric mind tumours: a evaluate from the Hospital for Sick Children. Natural history of meningioma development in mice reveals a synergy of Nf2 and p16(Ink4a) mutations. Parental occupation and childhood brain tumors: astroglial and primitive neuroectodermal tumors. Tumors of the nervous system and pituitary gland related to atomic bomb radiation exposure. An worldwide case�control research of adult glioma and meningioma: the position of head trauma. Significant association of a number of human cytomegalovirus genomic loci with glioblastoma multiforme samples. Nf1;Trp53 mutant mice develop glioblastoma with evidence of strain-specific effects. Haploinsufficiency of Snf5 (integrase interactor 1) predisposes to malignant rhabdoid tumors in mice. Investigation of human brain tumors for the presence of polyomavirus genome sequences by two impartial laboratories. Primary lymphoma of the central nervous system: epidemiology, pathology and current approaches to diagnosis, prognosis and therapy. Distant sequelae of traumatic brain harm: untimely mortality and intracranial neoplasms. Direct sequencing analysis of transmembrane area of human Neu gene by polymerase chain reaction. Occupational risk components for mind tumors: outcomes from a population-based case�control research in Germany. A collaborative study of cancer incidence and mortality amongst vinyl chloride workers. Nitrate in consuming water: a case�contol examine on primary brain tumours with an embedded ingesting water survey in Germany. The histopathology and ultrastructure of simian adenovirus 7-induced intracranial neoplasms. Grave cranio-cerebral trauma 30 years ago as reason for the brain glioma on the locus of the trauma: particulars of the case. Mouse fashions to interrogate the implications of the differentiation status in the ontogeny of gliomas. Epidemiological examine of major intracranial tumors: a regional survey in Kumamoto prefecture in southern Japan-20-year study. New primary neoplasms of the central nervous system in survivors of childhood most cancers: a report from the Childhood Cancer Survivor Study. Potential danger components for incident glioblastoma multiforme: the Honolulu Heart Program and Honolulu-Asia Aging Study. More about: cell and molecular biology of simian virus forty: implications for human infections and disease. Establishing intracranial mind tumor xenografts with subsequent analysis of tumor growth and response to remedy utilizing bioluminescence imaging. Incidence of neoplasms in ages 0�19 y in parts of Sweden with high 137Cs fallout after the Chernobyl accident. Second intracranial neoplasms following treatment of childhood acute lymphoblastic leukaemia. IgE, allergy, and threat of glioma: update from the San Francisco Bay Area Adult Glioma Study within the temozolomide period. Reduced allergy and immunoglobulin E amongst adults with intracranial meningioma in comparability with controls. An updated pooled analysis of glutathione S-transferase genotype polymorphisms and risk of grownup gliomas. They embody the frequent diffusely infiltrative astrocytomas, as properly as the much less common, low-grade circumscribed variants. Also characteristic are preferential location within the cerebral hemispheres, extra frequent presentation in adults than youngsters, and a variety of histopathological options, genetic alterations and organic behaviour. Interestingly, diffuse astrocytomas not often contain the cerebellum as a major website. In children, the brain stem and thalamus are characteristic locations for diffuse 1638 Overview and Biology of Diffuse Astrocytic Tumours 1639 astrocytomas. Pilocytic astrocytomas arise most regularly within the cerebellum, mind stem, optic pathways and hypothalamus. Non-localizing indicators and signs are also common, notably headaches, seizures and altered consciousness. In the setting of lower-grade lesions, seizures could also be current for years before the onset of different medical indicators and symptoms. Ultimately, sufferers develop elevated intracranial strain owing to mass effect. Most glioma classifications have postulated that astrocytomas arise from astrocytes, and oligodendrogliomas from oligodendrocytes. Significant indicators of accelerating grade in gliomas include cytological atypia, mobile density, mitotic activity, microvascular proliferation and necrosis. Importantly, both astrocytic differentiation and tumour grading are determined morphologically and subject to interpretation. A glioma progenitor cell may arise both from a stem cell inhabitants or from a differentiating progenitor cell inhabitants. Astrocytomas can develop via quite a few pathways of acquired gene mutations, amplifications and deletions. For occasion, overexpressing oncogenic Ras and Akt in progenitors leads to mouse mind tumours which are histologically similar to glioblastomas, but concentrating on more mature astrocytic progenitors is less oncogenic. Another gene related to chromatin transforming, H3F3A, is mutated in astrocytomas and appears to be an early event, mostly in paediatric high-grade astrocytomas. There are two kinds of recurrent somatic mutations that occur in H3F3A, with one leading to amino acid substitution at K27 and the other at G34. Mouse modelling research have proven variations in tumour morphology relying on the sort of cell transformed, in addition to the oncogenic mixture. Morphologically distinct areas in oligoastrocytomas have related genetic alterations, indicating that these are clonal lesions, albeit with hanging phenotypic variety. Nonetheless, as extra delicate neuronal markers are utilized, many glial neoplasms seemingly coexpress neuronal and glial antigens, either uniformly or focally. It is attention-grabbing to observe, nevertheless, that these oligodendroglial tumours with 1p and 19q loss preferentially affect specific areas of the brain, raising the chance that particular precursor populations in several brain areas transform along distinct genetic pathways to attain frequent phenotypic end points, corresponding to oligodendroglioma. Malignant glioma cells show preferential invasion alongside white matter tracts, around neurons and blood vessels, and within the subpial area. These infiltrative tendencies counsel that glioma cells have either a tropism for explicit sites or a restricted capacity to invade other regions. Moreover, glioma invasion is finest seen because the mixed ability to migrate and to modulate the extracellular space. Unfortunately, investigations of glioma invasion have been hampered by a paucity of representative experimental models that mimic the human illness. Invasion by glioma cells displays a dynamic interplay between cell�cell adhesion, remodelling of the extracellular matrix and cell motility. In common, the extracellular matrix of the mind is ill outlined and scant, consisting primarily of hyaluronic acid, except in two areas: around blood vessels and at the pial surface (glia limitans). Investigations into astrocytoma invasion have highlighted the complicated nature of cell�cell and cell�extracellular matrix interactions. These degrade the extracellular environment to facilitate migration, but additionally remodel the environment in a way that facilitates tumour cell progress.
Two cells may form a microrosette acute gastritis symptoms nhs order 40 mg protonix otc, the lumen of which is crammed with these floor protrusions gastritis symptoms sore throat protonix 20 mg order with visa. The basal bodies of cilia are simple to discern as the traditional 9 + 2 triplets diet for gastritis and duodenitis 40 mg protonix buy amex, which give rise to the axial fibrils of cilia. The third characteristic is the presence of advanced intercellular junctions similar to those of regular ependyma. Although the presence of these ultrastructural features is useful in the analysis, the overwhelming majority of ependymomas may be diagnosed with out electron microscopy. However, in individual instances missing decisive morphological and immunohistochemical features, electron microscopy may be useful. Nevertheless, rare tumours may also lack typical ultrastructural features and current problems even ultrastructurally. However, small biopsy specimens or the presence of intensive secondary adjustments, however significantly the histological variants of mobile, clear cell, tanycytic and papillary ependymomas, may pose differential diagnostic problems. Cellular ependymoma shows a conspicuous cellularity however, in contrast to anaplastic ependymoma, lacks additional options of anaplasia. Clear cell ependymomas may be troublesome to distinguish from oligodendrogliomas, central neurocytomas and metastatic renal cell carcinomas. Furthermore, clear cell ependymomas differ from oligodendrogliomas by their non-infiltrative progress. Thus, staining for neurofilaments often shows no or solely few residual axons within the tumour. In distinction to clear cell ependymoma, central neurocytomas are diffusely optimistic for synaptophysin, usually categorical NeuN focally, and ultrastructurally present proof of neuronal differentiation, together with dense secretory granules, progress cones and synaptic buildings. Tanycytic ependymoma may be difficult to distinguish from an astrocytoma, in particular as a result of perivascular pseudorosettes are sparse. However, different options of pilocytic differentiation are absent and ultrastructural investigation reveals ependymal traits. Some resemble schwannoma, however differ in their intramedullary localization and lack of dense intercellular reticulin or basement membrane deposition. Papillary ependymomas ought to be distinguished from different papillary tumours, together with metastatic carcinomas, choroid plexus tumours, papillary pituitary adenomas, astroblastomas, papillary tumours of the pineal area and papillary meningiomas. Furthermore, the perivascular pseudorosettes of ependymomas resemble these of astroblastomas, albeit with a more distinctly fibrillar quality. Choroid plexus tumours are constructive for cytokeratins, that are often unfavorable in ependymomas and astroblastomas. Immunoreactivity for prealbumin (transthyretin) and a variety of other novel choroid plexus markers, such as Kir7. In paediatric ependymomas of the posterior fossa, medulloblastoma represents an necessary differential diagnosis. Furthermore, the neuropil-rich Homer Wright rosettes in medulloblastoma are distinct from ependymal rosettes or pseudorosettes, although the latter may be seen in medulloblastomas as properly. Furthermore, stem-like most cancers cells isolated from ependymomas displayed a radial glia phenotype and have been capable of generate ependymomas when transplanted into nude mice. Moreover, activation of ephrinB2 signalling in these particular neural stem cells resulted in the first transgenic mouse model for ependymoma. It stays to be shown whether or not this speculation holds true for all ependymoma subtypes or whether other cell varieties. Molecular genetics A evaluation of conventional cytogenetic findings in one hundred twenty five ependymal tumours revealed irregular karyotypes in 83 (66 per cent), of which 24 had a sole autosomal abnormality. Structural abnormalities of chromosomes 1, 6 and 17, and numerical abnormalities of chromosomes 7, 9, 12 and 20 had been additionally noted. Spinal intramedullary ependymomas preferentially demonstrate losses of 1700 Chapter 29 Ependymal Tumours chromosomes 22q and 14q and features on chromosomes 7q, 9p and sixteen. In contrast, intracranial ependymomas incessantly carry positive aspects of 1q and losses on 6q. Among the assorted genomic imbalances, gains on 1q have been correlated with the presence of structural chromosomal aberrations, paediatric age, high-grade histology and aggressive clinical behaviour. Group B tumours (favourable prognosis) are genetically more unstable with frequent gains and losses on numerous chromosomes. Most of these tumours are situated within the cervical cord, with multifocality being common. In basic, spinal intramedullary ependymomas in adults are related to long-term, recurrence-free and overall survival after complete resection. A European population-based analysis estimated a 5-year overall survival fee of eighty three. This is in addition to biological elements, corresponding to affected person age, tumour location, illness dissemination, histological grade and sure immunohistochemical and molecular parameters (see earlier). Surgery is an important variable, with full resection being the most effective predictor of favourable prognosis in sufferers with localized disease. Another evaluation of 1011 youngsters with main intracranial tumours recognized extraneural metastases in solely 10 (0. Anaplastic ependymomas are notably prevalent in kids and are much more common among intracranial lesions, specifically infratentorial lesions, as in comparison with spinal lesions. Histologically, the tumours are characterized by options of anaplasia, particularly excessive mitotic exercise and elevated cellularity, usually in conjunction with microvascular proliferation and areas of pseudopalisading necrosis. In distinction to malignant astrocytic and oligodendroglial tumours, most anaplastic ependymomas are nonetheless well-demarcated with solely limited invasion into adjacent parenchyma. However, extra extensive mind invasion is seen in rare instances, in particular in kids and young adults with intracerebral lots which are neuroradiologically indistinguishable from other malignant gliomas. In distinction to intracranial tumours, intraspinal ependymomas not often show anaplastic features. Cellular pleomorphism could also be striking, together with the presence of enormous atypical and even multinucleated large cells. On the opposite hand, poorly differentiated, small anaplastic cells may predominate in some tumours, eliciting a differential diagnosis with embryonal tumours. Perivascular pseudorosettes are normally recognizable in anaplastic ependymoma whereas different features of well-differentiated ependymoma, similar to ependymal rosettes, ependymal tubules and clefts lined by ependymal cells are sometimes absent. Areas of tumour necrosis may be extensive, and glioblastoma-like options, similar to pseudopalisading necrosis and/or microvascular proliferation are often current. In anaplastic ependymomas with marked microvascular proliferation and pseudopalisading necrosis, the differential diagnosis of glioblastoma can come up. Nevertheless, a subset of anaplastic ependymomas is frankly invasive and occasional glioblastomas present perivascular pseudorosettelike architectures reminiscent of ependymal differentiation. In such cases, consideration of scientific options, similar to affected person age and tumour location, might present helpful clues. In rare instances, ultrastructural options of ependymoma or a molecular signature of glioblastoma resolves this differential. Histologically, myxopapillary ependymoma is characterised by tumour cells forming papillary buildings round vascular mucoid stromal cores. Among 298 ependymomas collected from completely different institutions, 13 per cent corresponded to the myxopapillary type. In addition, sufferers are normally treated with adjuvant radiotherapy and/or chemotherapy. Myxopapillary Ependymoma 1703 localization and Macroscopy Myxopapillary ependymomas are virtually solely positioned within the region of the conus medullaris, cauda equina and filum terminale. Rare instances have been reported in different areas, including the cerebral hemispheres,80 cerebral ventricles,37 cerebellopontine angle,seventy five medulla oblongata,eleven thoracic�cervical spinal cord, and spinal nerve roots. Macroscopically, the tumours are solitary, lobulated and infrequently encapsulated, gentle, greyish and translucent lesions. Large growths may compress and even envelop the cauda equina, however invasion of the nerve roots is uncommon: these cases present surgical difficulties. Occasionally, myxopapillary ependymoma may come up along side malformative lesions corresponding to tethered twine, dermal sinus and dermoid cyst. Abundant microtubular aggregates inside tough endoplasmic reticulum have been detected in some cases and will symbolize a unique feature. Other tumours that must be thought-about embody chordoma, myxoid (chordoid) chondrosarcoma, mesothelioma and metastases from adenoid cystic carcinoma or mucinous adenocarcinoma.
Histologically gastritis nuts protonix 40 mg generic line, focal parakeratosis chronic gastritis low stomach acid protonix 40 mg order mastercard, cytoid bodies in the cornified and granular layers gastritis diet 7 up cake 20 mg protonix buy fast delivery, the presence of eosinophils and plasma cells within the inflammatory infiltrate, and an infiltrate across the deep vessels favor a prognosis of lichenoid drug eruption. The latent period may be shortened if the patient has been beforehand exposed to the drug. Rechallenge with the culprit drug has been tried in a few patients, with reactivation of symptoms inside 4�15 days. Drugs are a wellknown reason for cutaneous pseudolymphomas (see Chapter 146), however the condition may be induced by foreign agents such as insect bites, infections. The eruption typically manifests as single lesions but can be widespread erythematous papules, plaques, or nodules. Most patients even have fever, marked lymphadenopathy and hepatosplenomegaly, and eosinophilia. Urticaria is normally a manifestation of small vessel vasculitis, with individual lesions remaining mounted in the identical location for more than 1 day. Other options embrace hemorrhagic bullae, ulcers, nodules, Raynaud disease, and digital necrosis. The similar vasculitic course of may also affect internal organs such as the liver, kidney, intestine, and central nervous system and may be potentially life threatening. In some cases, serologic testing has revealed the presence of perinuclear-staining antineutrophil cytoplasmic autoantibodies in opposition to myeloperoxidase. Alternative causes for cutaneous vasculitis corresponding to infection or autoimmune disease must be eliminated. Tissue eosinophilia could additionally be an indicator of drug induction in cutaneous small vessel vasculitis. Circulating anti-Ro (Sj�gren syndrome A) antibodies have also been identified in plenty of sufferers. Many medicine have been implicated in causing druginduced lupus syndromes, especially hydralazine, procainamide, isoniazid, methyldopa, and minocycline. The variety of patients who develop subacute cutaneous lupus erythematosus throughout therapy with these medications is very low, and these medicine are thought to have a low danger for causing or exacerbating cutaneous lupus. Cutaneous findings embody livedo reticularis, painful nodules on the legs, and nondescript eruptions. A drug cause must be thought-about in the differential prognosis of a large spectrum of dermatologic ailments, particularly when the presentation or course is atypical. The diagnosis of a cutaneous drug eruption includes the exact characterization of reaction sort. A broad variety of cutaneous drug-associated eruptions may warn of related internal toxicity (Table 41-3). The most typical serologic abnormality is positivity for antinuclear antibodies with a homogenous sample. Fever, malaise, pharyngitis, and other systemic symptoms or indicators must be investigated. A usual screen would come with a full blood depend, liver and renal function tests, and a urine analysis. Skin biopsy must be thought-about for all sufferers with doubtlessly extreme reactions, similar to these with systemic symptoms, erythroderma, blistering, skin tenderness, purpura, or pustulation, as nicely as in circumstances by which the prognosis is uncertain. Instead, diagnosis and evaluation of cause involve analysis of a constellation of features similar to timing of drug exposure and reaction onset, course of reaction with drug withdrawal or continuation, timing, and nature of a recurrent eruption on rechallenge, a history of an identical response to a crossreacting medication, and former stories of comparable reactions to the identical treatment. Several in vitro investigations may help to confirm causation in particular person cases, however their exact sensitivity and specificity stay unclear. Investigations embody the lymphocyte toxicity and lymphocyte transformation assays. Patch testing has higher sensitivity if performed over a previously involved space of skin. However, a reaction suggestive of a probably life-threatening scenario should prompt immediate discontinuation of the drug, along with discontinuation of any interacting drugs that will gradual the elimination of the suspected causative agent. Although the function of corticosteroids in the treatment of great cutaneous reactions is controversial, most clinicians choose to begin prednisone at a dosage of 1�2 mg/kg/day when symptoms are extreme. Antihistamines, topical corticosteroids, or each can be used to alleviate signs. Drug desensitization, also referred to as induction of drug tolerance, has been used primarily for IgE-mediated reactions attributable to medication similar to penicillin or more recently, monoclonal antibodies such as rituximab and infliximab. However, as soon as a response has occurred, it is essential to stop future similar reactions within the affected person with the identical drug or a cross-reacting medicine. Some of those may be inherited, which places firstdegree family members at a larger risk than the final population for the same response to the same or a metabolically cross-reacting drug. Postmarketing voluntary reporting of uncommon, extreme, or unusual reactions stays essential to enhance the safe use of pharmaceutical brokers. Eshki M et al: Twelve-year evaluation of extreme instances of drug response with eosinophilia and systemic signs. Mockenhaupt M: Severe drug-induced skin reactions: Clinical pattern, diagnostics and remedy. Justiniano H, Berlingeri-Ramos A, Sanchez J: Pattery evaluation of drug-induced skin illnesses. Most usually begins as a single 2- to 4-cm skinny oval plaque with a fantastic collarette of scale located contained in the periphery of the plaque ("herald patch"). Similar-appearing, however smaller, lesions appear a number of days to weeks later, typically distributed alongside the traces of cleavage on the trunk ("Christmas tree" pattern). Treatment is often supportive, though midpotency topical corticosteroids can reduce pruritus; high-dose acyclovir for 1 week may hasten recovery. The preliminary lesion is adopted a quantity of days to weeks later by the appearance of quite a few similar-appearing smaller lesions positioned along the strains of cleavage of the trunk (a so-called Christmas tree pattern). As properly, the characteristic distribution of lesions and variations in lesional and nonlesional pores and skin are unexplained. In a minority of patients, flu-like signs have been reported, together with basic malaise, headache, nausea, loss of urge for food, fever, and arthralgias. In roughly 20% of patients, the scientific image diverges from the basic one described above. Localized types of disease could involve colored, erythematous, or hyperpigmented (especially in individuals with darker skin); and demonstrates a fine collarette of scale simply contained in the periphery of the plaque. The interval between the looks of the primary plaque and the secondary eruption can range from 2 days to 2 months, but the secondary eruption typically happens inside 2 weeks of the looks of the primary plaque. The secondary eruption happens in crops at intervals of a few days and reaches its maximum in approximately 10 days. The symmetric eruption is localized primarily to the trunk and adjacent regions of the neck and proximal extremities. The most pronounced lesions extend over the abdomen and anterior floor of the chest as nicely as over the back. Two major kinds of secondary lesions occur: (1) small plaques resembling the primary plaque in miniature, aligned with their long axes alongside lines of cleavage and distributed in a Christmas tree sample, and (2) small, pink, usually nonscaly papules that gradually enhance in number and spread peripherally. The palms and soles are involved at times, and the scientific picture in these patients could simulate a widespread eczematous eruption. Typical histopathologic features embody focal parakeratosis, a reduced or absent granular cell layer, mild acanthosis, mild spongiosis, papillary dermal edema, a perivascular and superficial dermal interstitial infiltrate of lymphocytes and histiocytes, and focal extravasation of erythrocytes. The histologic image is indistinguishable from that of superficial gyrate erythema. In older lesions, the perivascular infiltrate is usually both superficial and deep, with much less spongiosis and extra pronounced acanthosis. These late lesions may be difficult to distinguish from psoriasis and lichen planus. However, leukocytosis, neutrophilia, basophilia, lymphocytosis, and slight will increase in erythrocyte sedimentation price and ranges of whole protein, 1- and 2-globulins, and albumin have been reported. Pityriasis lichenoides chronica could current with a Christmas tree sample on the trunk, however as a rule, typical lesions might be found on the extremities. These include arsenic, barbiturates, bismuth, captopril, clonidine, gold, interferon-, isotretinoin, ketotifen, labetalol, organic mercurials, methoxypromazine, metronidazole, omeprazole, d-penicillamine, salvarsan, sulfasalazine, terbinafine, lithium, and tripelene amine hydrochloride.
Unlike acute/ lively and chronic energetic plaques gastritis diet livestrong protonix 40 mg order mastercard, these lesions are not the sites of inflammatory demyelination and gastritis pain treatment generic 40 mg protonix fast delivery, therefore gastritis diet ��������� buy protonix 20 mg cheap, symbolize the end levels of immunopathological damage. These options are reflected in all the plaque classification techniques the place the inactive lesion figures. Plaques may turn out to be extra visible in the cut sections after exposure to air for a while. The dimension and anatomical location of a lesion and the intensity of the previous inflammatory course of are more doubtless to be among the many components that contribute to variability in temporal evolution of lesions; it has been estimated that it takes 18 months or longer for an lively plaque to purchase this appearance. Because myelin lipid components are only slowly and partially catabolized in macrophages, foamy macrophages might persist in them for lengthy durations. In basic, mature oligodendrocytes are most often utterly lost in inactive plaques. The mechanisms of neurodegeneration in these continual inactive lesions could also be totally different from those operative in acute lesions, in as much as 23. Chronic plaques (superior frontal and temporal lobe white matter) have sharp borders. Interestingly, the perivascular cuffs in the periplaque white matter contain almost exclusively lymphocytes, whereas within the plaque the cuffs comprise lymphocytes and cells of histiocytic origin, a proven fact that implicates the lymphocyte as being essential within the early pathogenesis of the lesion. Representative sections of continual lively plaques illustrating peri-plaque white matter (a,b), the demyelinating plaque edge (a�g), the intermediate zone between the plaque edge and centre (h,i) and the plague centre (j,k). The central area of the plaque (far right) is far much less cellular, and the diploma of cellularity progressively will increase centrifugally up to the plaque edge. Note the entire absence of myelin and the gradient of increasing hypercellularity from the area closest to the plaque centre (below) to that nearest the plaque edge (above). Electron micrograph showing two oligodendrocytes (O) related to axons (A) with thin (probably remyelinated) myelin sheaths. Processes from myelin debris-containing macrophages (lower left and upper right) are approaching and seem to be demyelinating a few of these myelin sheaths. Continual breakdown and regeneration of myelin in progressive multiple sclerosis plaques. Interestingly, the myelinated axons within the plaque edge, even in the persistent inactive state, should include long areas of redistribution of caspr from the paranode, as in the lively state. Haemosiderin and fibrin deposits related to plaque blood vessels and prominent amyloid deposition in plaque blood vessels have also been observed in rare instances. There are variable numbers of persistent lipid-laden macrophages, significantly in perivascular areas. As myelin is depleted, immune activation, in addition to phagocytosis lower, and the foamy macrophages themselves might contribute to a dampening of the immune response. Myelin phagocytes also seem around small blood vessels in comparatively preserved tissue, i. Such lesions are often large and could be located away from the ventricles; they may show ring enhancement or cystic change and will or could not trigger mass 1344 Chapter 23 Demyelinating Diseases 23. This is evident as pale brown perivenular extensions of a plaque involving the wall of the lateral ventricle in (d) (small arrows). In very continual cases periventricular white matter plaques may be fairly distinguished, extending deep into the hemispheric white matter (b). In addition to the plain white matter plaques, sometimes gray matter plaques, such as the one within the thalamus in (e) (arrow), may be appreciated on gross examination. Spinal cord plaques can also be evident macroscopically, as proven at two levels in the left lateral funiculus of the cervical twine in (f) and (g). Advanced imaging techniques and repeated examinations could present information extra suggestive of inflammatory/demyelination,123,206 but biopsy sampling for analysis may be essential to determine the character of the lesion. In the vast majority of circumstances, these tumefactive lesions are solitary and located within the cerebrum. They can, nevertheless, even be a quantity of and may be in different websites, such because the cervical spinal twine, and associated with a clinically isolated syndrome. To the extent that the tissue pattern dimension permits, you will want to carry out research that rule out different pathological processes, significantly infection, infarction and neoplasia (see Table 23. Reactive features, together with inflammation and astrocytosis, could additionally be seen adjacent to lesions with an entirely totally different aetiology, for example abscesses and infarcts, the diagnostic parts of which is probably not included within the sample. A number of histological options can help within the distinction of inflammatory demyelination from other pathological processes. Many plaques are periventricular, but some are extra peripheral within the corona radiata. The giant plaque on the right encompasses approximately one-third of the cross-sectional area of the twine, including gray matter, at this degree. There is additional myelin pallor past the boundaries of the plaques that may characterize tract degeneration and/or ongoing disease activity. Note the immunostaining of spinal nerve roots in addition to intact myelin within the cord. Courtesy of Dr G Wolswijk, Netherlands Institute for Brain Research, Amsterdam, the Netherlands. The demonstration of myelin loss, utilizing myelin stains, and relative preservation of axons, often by silver impregnation techniques or neurofilament immunohistochemistry, is crucial for the diagnosis of a demyelinating process. Some axons appear injured and axonal numbers could additionally be partially depleted, but their loss ought to be comparatively less than that of myelin. If axons are depleted to the identical extent as myelin, or if gray matter with hypoxic�ischaemic neurons is current within the pattern, the lesion is extra prone to be an infarct or other necrotizing process than demyelination. A predominance of B-cells is unusual and raises the possibility of a lymphoproliferative disorder. Large numbers of neutrophils, fibrinoid necrosis of vessels and intravascular thrombi also suggest various illness processes similar to an infection and vasculitis. In the absence of scientific and neuroimaging knowledge and, specifically, data of the temporal evolution of the lesion, a precise analysis primarily based on the findings of an acute inflammatory demyelinating lesion will not be potential. Another caveat is that in rare situations, demyelination could be observed adjoining to a non-demyelinating lesion, similar to a neoplasm641 or might herald a lymphoma. In every of the panels, the plaque is on the proper and the adjoining white matter on the left. There is a relative discount in the numbers of oligodendrocytes, that are ample in the adjacent white matter (a�d, black arrows). Gliosis is manifest within the plaque by astrocytes with fibrillary processes (a,b, white arrows). The Bielschowsky stain demonstrates lesional axonal loss (g,h); the surviving axons are less intensely impregnated with the silver salt than their counterparts in the adjoining white matter (g,h). These lesions can, nevertheless, be quite in depth, involving giant areas of the cortex. Note the thinly myelinated axons on the plaque border (centre of figure), fibrous astrocytes and microglia (arrowheads). The perivascular house contains many thin-walled channels during which there are lymphocytes (L) and macrophages (M); plasma cells (arrows) are situated exterior the channels. Surface contacts of lymphocytes with macrophages might result in antigen presentation. Cortical lesions were described as hypocellular, with only a few inflammatory cells,365 the numbers of T- and B-lymphocytes being no different in nondemyelinated and control regular cortices. They are present in increased numbers all through and at the borders of energetic lesions, however not in chronic silent cortical lesions or regular cortex. Although this pattern is just like that in white matter plaques, microglia in cortical plaques retain their rod-like shapes, whereas in white matter plaques most have matured into spherical phagocytic macrophages. Nevertheless, the activated microglia, that have been shown to produce myeloperoxidase277 could still be capable of inflicting damage on myelin and neurons, as their processes are intimately related to neuron cell our bodies and neurites. Moreover, the cortical plaques additionally included macrophages that contained lipid or myelin breakdown products. Despite the restricted measurement of the pattern, the myelin stain demonstrates both perivascular and confluent areas of inflammatory demyelination. The space in the black rectangle is proven at larger magnification in (b), the place the demyelination is seen to extend for variable depths (double-headed arrows) into the cortex. Bielschowsky silver impregnation (e) reveals axonal loss within the areas of white matter demyelination however not within the cortex; nonetheless, larger magnification would show proof of transected neurites in cortical plaques.






